Vaccines, a proven protection against pathogens in our environment
PDF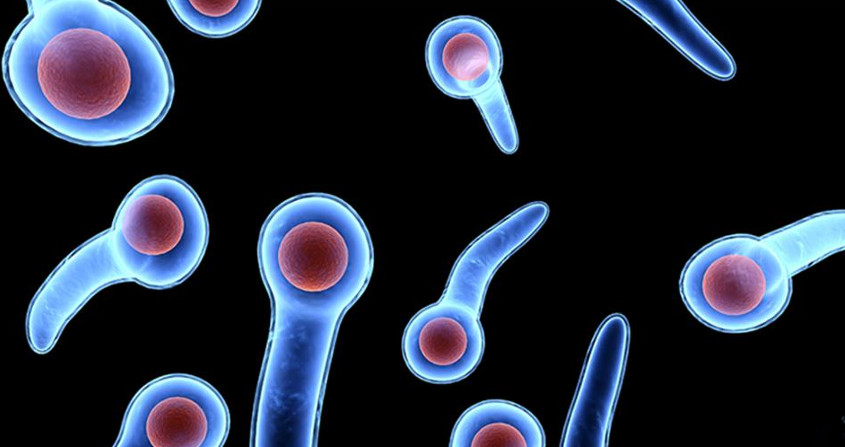
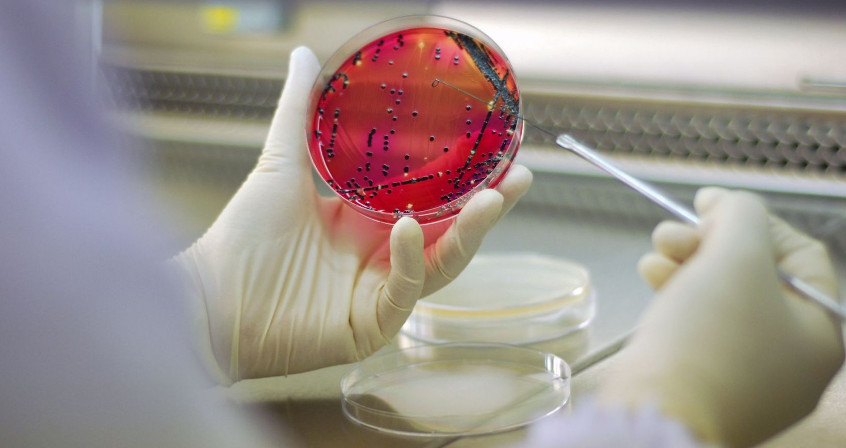
This article offers a series of reflections on an increasingly critical society with regard to vaccines. Vaccines, which are one of the most beautiful scientific discoveries in the history of mankind, are now causing controversy in developed countries. “Prophylactic” vaccination is an essential means of prevention against a number of infectious diseases. Some of these diseases can be strictly human (hepatitis B, measles, bacterial meningitis), others originate in the environment: tetanus (soil contaminated with excrement) – see above image- or poliomyelitis (contamination with water and food contaminated with water). Even diseases as common as influenza can have an environmental origin (pandemic influenza strains come from avian and swine strains). We present here the history of these oppositions and resistances to vaccination, which were born with the first public health measures in the 19th century in England where they took violent forms. Then we analyze the current controversies over vaccines. Finally, we analyse the consequences of the decline in vaccination, before looking at how the balance between mandatory and recommended vaccines is struck.
Vaccination killed four doctors in a Pakistani province one morning in November 2014. These precious health workers did not die from the vaccine, but under bullets of Kalashnikovs from the Taliban who had sentenced them to death for the “crime of spreading a non-Islamic vaccine”. The small group of vaccinators had just arrived on board 4x4s in this small border village as part of the WHO polio eradication programme. These doctors went around the countryside, knocking on doors, begging mothers to let them approach their children to make them drink a few drops of the precious vaccine. Pakistan remains one of the last three countries in which polio is still prevalent along with Nigeria (in which vaccinators have also been murdered). Pakistan accounts for 85% of the unfortunate cases of poliomyelitis, a viral disease that causes muscle paralysis and can kill by respiratory paralysis. This disease should no longer affect a single child, as there are several effective vaccines.
This bloody fact illustrates by its radicality and violence the problems and oppositions that vaccines have caused since the beginning of their history. These Pakistani doctors are not the first victims of obscurantist revolts in the short history of vaccines. Vaccination campaigns have generated conflicts and resistance since their inception. Not all oppositions are as radical or completely unfounded, but they are rooted in the same societal sources.
But the result of vaccination resistance is always the same, and the victims are most often children. Thus, measles reappeared in France in epidemic form between 2008 and 2012. It killed 10 people, caused 23,000 (reported) cases and more than 5,000 patients had to be hospitalized for complications. Three cases of severe tetanus have been reported since 2012 in children in France. In June 2015, an 8-year-old child was rushed to hospital in Tours. He had contracted tetanus after falling on a piece of pottery. He stayed 3 weeks in intensive care for a disease that should never have touched him. The paediatrician, with the consent of the parents, had written him a false vaccination certificate. The doctor has since been removed from the General Medical Council and banned from practice.
In this article, we will first analyse the history of opposition to vaccination, before considering the causes of current resistance, then discussing in a last part the balance between obligations and recommendations.
1. Vaccine resistance: the product of a long history
1.1. Mockery of the first vaccines

It should be remembered that smallpox is an eruptive viral infectious disease that already affected Egyptians (mummies display scares of infection). This millennial scourge struck all social classes alike (Louis XV succumbed to it in the small Trianon) and caused terrible epidemics. Smallpox killed half the patients it infected, left monstrous scars on those who survived it. Until the middle of the 20th century, it caused two million deaths annually and infected 50 million people [1].
But mockery turned into outright opposition, even bloody revolt, when vaccines were used as public health tools. They appeared as soon as the first laws imposing a vaccination obligation were drafted. They reflect social tensions, the complex relationships between obligation, state authority and individual freedom.
1.2. Very deep roots going back to Jennerian England
England, Edward Jenner’s homeland, was the first country in the world to introduce compulsory vaccination in 1853. The laws imposed significant fines or jail time for parents who did not vaccinate their children. At that time, the country was poor, the health system non-existent, and epidemiological surveillance was almost non-existent. Vaccination coverage rates were not sufficient to control epidemics. The non-vaccinated were the poorest and vaccination followed a social divide in English society between rich and poor.
In 1867, in view of the relative ineffectiveness of the law, the obligation was reinforced for all children over 14 years of age. Vaccinators visited the homes to verify that children on the birth records were properly vaccinated. The law was further consolidated in 1871. Vaccinators had to send the vaccination certificates that were checked against the birth certificate register. The effect of the law was relatively effective, although costly for the state that maintained the system. But the population was less and less tolerant of state interference in personal affairs. These laws were experienced as an attack on individual freedom.
In 1876, in Keighley, Yorkshire, vaccinators were arrested and briefly imprisoned in York by rioters. Anti-vaccine leagues were formed. In 1886, in Leicester, more than 6,000 people were prosecuted for lack of vaccines. Demonstrations by more than 20,000 people led to the discontinuation of the proceedings. The Leicester area became the spearhead of vaccine control in England [2]. Under the influence of the riots, English legislation was softened in 1895. Vaccine exemption was allowed in the form of a conscience clause. The law allowed citizens to refuse vaccination.

1.3. Vaccine resistance worldwide
1.4. France: a singular case
France represents a special case in terms of opposition to vaccination. Thus, vaccines did not crystallize any major opposition during the 19th and early 20th centuries. Several factors may have played a role. First of all, it is not unrelated to the fact that France lived under the tutelary shadow of Louis Pasteur (1822-1895), the “father of modern vaccines”. Pasteur victory over death and disease received all the honours a republic can offer. He was entitled to a national funeral. In Paris, Pasteur has his institute, his boulevard, his metro station. Even today, there is not a village in France that does not have its place, its street, its avenue Louis Pasteur. In the french republican imaginary, the vaccine is the embodiment of progress. It may seem like a smile, but it is a reality that Pasteur’s work has been traced in a furrow that deeply marked France with its flagship Institute in Paris, its worldwide network of institutes that spread science and participated in the great vaccination epic.

1.5. Where do we stand today?
Distrust of vaccines is a general phenomenon that is constantly increasing in developed countries for many reasons [4]:
- In developed countries, infectious diseases have declined so much in less than a generation (thanks to the success of vaccines) that the feeling of infectious danger has almost disappeared;
- Vaccines, (like all drugs) are likely to cause side effects, as modern epidemiology reveals, so they generate fears;
- Finally, vaccines are single drugs that are administered to healthy people. The occurrence of adverse effects is difficult to tolerate in such a context;
- More recently, there has been a suspicion of conflicts of interest or complicity between policy makers and vaccine manufacturers.
This is why anti-vaccine discourse is gaining ground, especially in France. In an international study published in 2016 on the study of confidence in the population, France took the lead in countries in which confidence in vaccines is falling dangerously [5]. In this study, 41% of respondents did not trust vaccines, placing France just ahead of Bosnia and Herzegovina (36%), while the international average of distrust was around 13%.
Governments were deeply concerned about these disappointing results. In recent years, several parliamentary reports have been issued on the vaccination policy to be adopted, in particular to achieve the vaccination coverage targets for the control of common infectious diseases. A major national consultation was launched, which produced its report at the end of 2016 [6]. In the recommendations of the consultation report, the extension of the obligation to all vaccines in the infant calendar is included. It is the famous “11 vaccines” that are now mandatory since January 2018.
2. Vaccine resistance and controversies
2.1. Old accidents with dramatic consequences
Beyond these circumscribed and well-known examples, the recent history of controversies over modern vaccines reports either analyses with no proven scientific basis or cases of real malfeasance.
2.2. The hepatitis B vaccine: a French example
Hepatitis B is a real public health problem. In France today, nearly 280,000 patients suffer from chronic hepatitis B and the hepatitis B virus (HBV) is responsible for the death of 1,500 patients per year. Globally, an estimated two billion people have been infected with the virus (almost one-third of the world’s population), and according to WHO in 2016, 257 million people were infected with chronic hepatitis B, resulting in 887,000 deaths. The disease is transmitted sexually, through exposure to contaminated blood, and during pregnancy from mother to child (transmission of between 40 and 90% of untreated cases). The hepatitis virus infects the liver and causes acute hepatitis (clinically in the form of jaundice), and in rare cases fulminant hepatitis: it is a death of the liver cells (necrosis) whose only treatment is liver transplantation. Finally, it is complicated by chronic hepatitis in 5% of cases. The virus then persists in the blood. Chronic hepatitis B slowly progresses for months or even years to cirrhosis and liver cancer.
To give an idea of the danger of this virus, HBV is 50 to 100 times more contagious than human immunodeficiency virus (HIV). It can be transmitted in everyday life by equipment contaminated by traces of blood (nail clippers, razors, earrings, etc…) or by poorly disinfected equipment used by professionals (acupuncture, tattoo parlours, piercing…). In France in 1990, it was estimated that there were more than 20,000 new infections annually.
France decided to launch an HBV vaccination campaign targeting infants, adolescents and adults at risk. A few cases of neurological disorders with multiple sclerosis type have been described in the aftermath of hepatitis B vaccination in young adults. Associations were formed to consolidate patients’ complaints and take them to court. In 1998, the French Agency for the Health Security of Health Products (AFSSAPS, which has since become the ANSM, for Agence nationale du médicament et des produits de santé) launched several scientific studies. This suspicion had only been reported in France and nowhere else in the world. In the autumn of 1998, under pressure from the media and associations, the Minister of Health decided to suspend the vaccination of adolescents in the sixth grade.
Since this suspension, all studies have consistently shown that there is no biological correlation between hepatitis B vaccination and multiple sclerosis. There was just a simultaneity, since the vaccines had been administered to young adults during the natural onset of multiple sclerosis. There was no causal link. The safety profile of hepatitis B vaccines is excellent given the safety and pharmacovigilance data and the decline over more than thirty years [7], [8]. Several billion doses of hepatitis B vaccine have been safely used.
The suspension of vaccination of adolescents in 1998 in France had negative public health effects, since these cohorts of young people are now in the age groups at risk of sexual exposure without any protection. It has been calculated that the continued vaccination of these adolescents would have prevented 1,000 acute hepatitis, 100 chronic hepatitis, and 5 fulminant hepatitis cases each year.
In the case of the hepatitis B vaccine, the health alert resulted in a health mess as a result of the overly broad use of the precautionary principle (see focus The precautionay principle).
2.3. Aluminium additives in France
In France, the safety of aluminium used in vaccines as an adjuvant has been the subject of considerable controversy since 1998. Professor Romain Gherardi (at Créteil) threw a stone into the pond by publishing an article in the famous magazine The Lancet. This article described a new muscle pathology in 18 patients: Macrophagic myofasciitis [9]. It showed that the microscars observed were associated with the presence of aluminum, a possible residue of the vaccine introduced by intramuscular injection. In 2003, the Romain Gherardi’s team linked macrophagic myofasciitis to a broader syndrome: chronic fatigue syndrome [10], [11]. The vaccine in question is again the one against hepatitis B widely used in adults in the 1990s.
These works were surprising in several ways:
- Aluminium has been used as an adjuvant in vaccines since 1925 with safety data collected from populations around the world. The decline in the safety of this component is therefore enormous, since several tens of billions of doses of vaccines have been administered since the beginning.
- Moreover, this syndrome was only found in France, and more precisely in patients of the Créteil team from which the cohort originated.
- Finally, it is children who are significantly exposed to vaccines with an aluminic adjuvant, and the cohort even extended to other patients was made up only of adults.
Nevertheless, this problem has long been taken very seriously by health authorities. The World Health Organization (WHO) addressed the problem in 1999 by setting up an advisory committee for vaccine safety, the first issue of which was the problem of aluminium-based adjuvants. In France, the Institut national de veille sanitaire (InVS) launched a pharmacovigilance study in 2002. Since then, many reports have been produced on the subject: in 2012, the Academy of Medicine, in 2013 the High Council on Public Health (HCSP), in 2014 the Parliamentary Office for the Evaluation of Scientific and Technical Choices, in 2016 the Academy of Pharmacy. The Academy of Pharmacy report stated that “given the heterogeneity and non-specificity of the clinical manifestations associated with histological lesion, it is not possible to define a macrophagic myofasciitis syndrome” [12]. The disorders observed concern only a few exceptional, even unique cases [13], which could correspond to very particular genetic predispositions. In any case, the potential risk is disproportionate to the benefits provided by this vaccine, as recalled by the ANSM.
2.4. Thiomersal and autism
Thiomersal is an organo-mercurial chemical compound with biocidal activity (i.e. it kills contaminating microbes). Thiomersal also helps to improve drug stability. These properties are useful for vaccination campaigns where multi-dose packaging is used (when one vial is used to vaccinate several people). Multiple doses are not administered simultaneously to several patients and the doses can therefore remain open without any risk of contamination.
In 1999, in the United States, the hypothesis that thiomersal exposure could be associated with neurodevelopmental deficits in children began to circulate [14]. These concerns were based on the calculation of the cumulative mercury intake in infant vaccination schedules, which may exceed the maximum rate recommended by the American authorities. From a toxicological point of view, the vaccines contained minimal doses of thiomersal, between 0.003% and 0.01%, with a maximum of 25 to 50 µg/dose. At these doses and in the situations of use any toxic risk was excluded a priori.
However, the Food and Drug Administration (FDA) has requested the withdrawal of thiomersal from all pediatric vaccines, which was effective in the United States and Europe in 2001. Detailed scientific work published in 2007 in the New England Journal of Medicine showed that there is no link between thiomersal and autistic disorders [15].
Again, many agencies have addressed the problem. The WHO in 2006, the European Medicines Agency (EMA) in 2007 and AFSSAPS in 2009, agree that the existence of neurological risk is not established (even if it cannot be scientifically excluded). Given these properties as an essential preservative in multi-dose vaccine presentations, the benefits of using thiomersal outweigh the theoretical toxicological risk.
2.5. Polio vaccine and the AIDS epidemic
In 1999, a book brought another controversy. The oral polio vaccine used in a 1959 vaccination campaign in Africa was reported to have caused the HIV pandemic [16]. The vaccine would have been produced on chimpanzee kidney cells that would have been contaminated with the simian immunodeficiency virus (SIVcpz) that would have been transmitted to humans and would have caused the group M immunodeficiency virus (HIV) and the global acquired immunodeficiency syndrome (AIDS) pandemic. The vaccine is normally produced on green monkey kidney cells (Vero cells) that do not carry chimpanzee SIV.
This hypothesis has been largely refuted by molecular comparison studies of the viruses [17], [18]. Therefore, it is not the oral polio vaccine that causes HIV. These results are supported by more recent data on the emergence of HIV. It appeared well before 1959 on the banks of the Congo River, since it was already circulating in Kinshasa in the 1930s [19].
2.6. The speech on over-vaccination
When the previous claims are scientifically proven one after the other, not without a public health cost, other more pernicious arguments emerge.
After the meaningless naturalistic discourse “better to be sick than vaccinated”, comes the argument that the vaccine makes you sick by tiring the immune system.
The multiplication of vaccines could lead to an over-activation of the immune system.
This idea is a scientifically false truth.
- On the one hand, because the vaccines have become more refined. It is estimated that twenty years ago there were about 3,000 antigens in all vaccines in the vaccination schedule. Nowadays, the number of these antigens has dropped to 150 [20]. But it must be understood that 3,000 or 150 antigens are a drop in the ocean of the 10,000 billion bacteria and viruses that surround us and against which our immune system has been constantly responding since birth. This represents a drop in the almost infinite possibilities of our immunological repertoire acquired during evolution. We are therefore far from saturating our immune system with our vaccination schedule [21].
- On the other hand, modern immunology teaches us that the stimulation of the immune system by the environment is necessary for the harmonious development of immunity [22] (see Human microbiotas: Allies for our health).
3. What public health policy?
3.1. The beneficial effects of vaccines
Epidemiologically, vaccines are a real success story. The incidence of vaccine-preventable diseases fell by 100% in the United States in the 20th century [23].
In France, similar results are observed. The last cases of indigenous polio and diphtheria were in 1989. The tetanus agent persists indefinitely in the soil thanks to its very resistant spores, it cannot be eradicated, but it is controlled to less than ten cases per year. Since the introduction of Haemophilus influenzae type b vaccinations in 1992, the incidence of meningitis has dropped by 96% among children under 5 years of age [24].
The benefits of vaccines can be quite surprising, in some cases exceeding the simple direct effect on the drop in the number of cases. Thus, the measles vaccine increases the lifespan beyond the simple protective effect it provides against measles-related mortality [25]. This “additional” benefit is related to the fact that measles infection is highly immunosuppressive and causes us to lose immunity to many other diseases. By protecting us against measles, the vaccine increases immunity to other diseases.
Pneumococcus is a bacterium that causes ear infections, meningitis and serious lung infections mainly at both ends of life: in children and the elderly. The pneumococcal vaccine introduced into the childhood immunization schedule dramatically reduces not only childhood ear infections and meningitis, but also pneumonia in the elderly (which are not vaccinated), reminding us (or finishing to show us) that children are the vectors of pneumococcal infections in the elderly. By interrupting pneumococcal transmission by vaccinating children, the vaccine directly protects children and indirectly protects the elderly around them. Vaccines against early childhood infections have indirect beneficial effects on antibiotic resistance by saving unnecessary prescriptions and reducing health costs.
In a word, vaccines reduce infections. But infectious diseases, under control, have not disappeared. They patiently wait for the opportunity of a drop in the vaccine shield to reappear mechanically.
3.2. The mechanical effects of the decline in immunization coverage
In 1900, life expectancy in France varied around 45 years. By 2016 it had risen to an all-time high of 79.4 years for men and 85.4 years for women. Vaccines are not the only cause of this dramatic increase in life expectancy, but they have been a major contributor.
The decline in vaccination mechanically induces like a pendulum game the return of pertussis, terrible diphtheria (it had reemerged in Russia with the fall of the Soviet empire), meningitis in young children, a resettlement of measles, mumps, rubella, and why not polio if it were reintroduced in Europe. Finally, it leads to an increase in antibiotic resistance following their massive use to treat bacterial complications of viral infections.

France launched a measles plan in 2005. Measles has become a notifiable disease. Cases were monitored by an epidemiological investigation at each report. In 2006, France had fewer than 50 cases per year, which is less than the target set by the WHO. Unfortunately, due to the decline in immunization coverage, a measles epidemic began in early 2008 and more than 23,000 cases were reported between 2008 and 2012. The epidemic has resulted in the hospitalization of almost 5,000 patients (1,023 severe viral or bacterial pneumopathies, 27 neurological complications such as encephalitis or myelitis), and 10 deaths, the majority of which were under 30 years of age. This upsurge had been predicted by modelling work due to insufficient measles vaccination coverage in France. While immunization coverage for the MMR infant vaccine has increased in recent years, it is still insufficient. It was 90% at one year for one dose, but dropped to 54% for two doses, while the elimination plan targets were 95% and 80%, respectively, for one and two doses.
This example illustrates that the guard can only be safely lowered if the disease has been completely eradicated worldwide. This is a long and complex operation that has been successfully carried out for smallpox. It is ongoing for polio and is being considered for measles. But it requires global coordination and very significant efforts. The eradication of a virus depends, as in a chain, on the resistance of its weakest link.
3.3. Obligation or recommendation?
Within the European Union, France shares with Italy the particularity of being one of the last countries to impose a vaccination obligation. This is the result of historical choices in the middle of the 20th century, at a time when infectious diseases were still causing considerable damage to the populations of these two countries.
For the legislator, it was a question of effectively combating serious diseases in a context of infectious risk. But since 1964, however, no new vaccines have been included in the vaccination schedule under the seal of obligation. These changes also correspond to societal changes in which the patient is more involved in the choices that concern him/her. The obligation appears to be in contradiction with the law of 4 March 2002 on the right of the patient and in particular the right to refuse treatment. The result is a great paradox in terms of the readability of the vaccination policy into which many opponents have rushed.
Mandatory vaccines seem less important in terms of interest since they protect against diseases that have disappeared in France (diphtheria, poliomyelitis), while vaccines simply recommended such as hepatitis B and human papillomavirus protect against diseases that kill 1,500 and 1,000 people respectively each year.
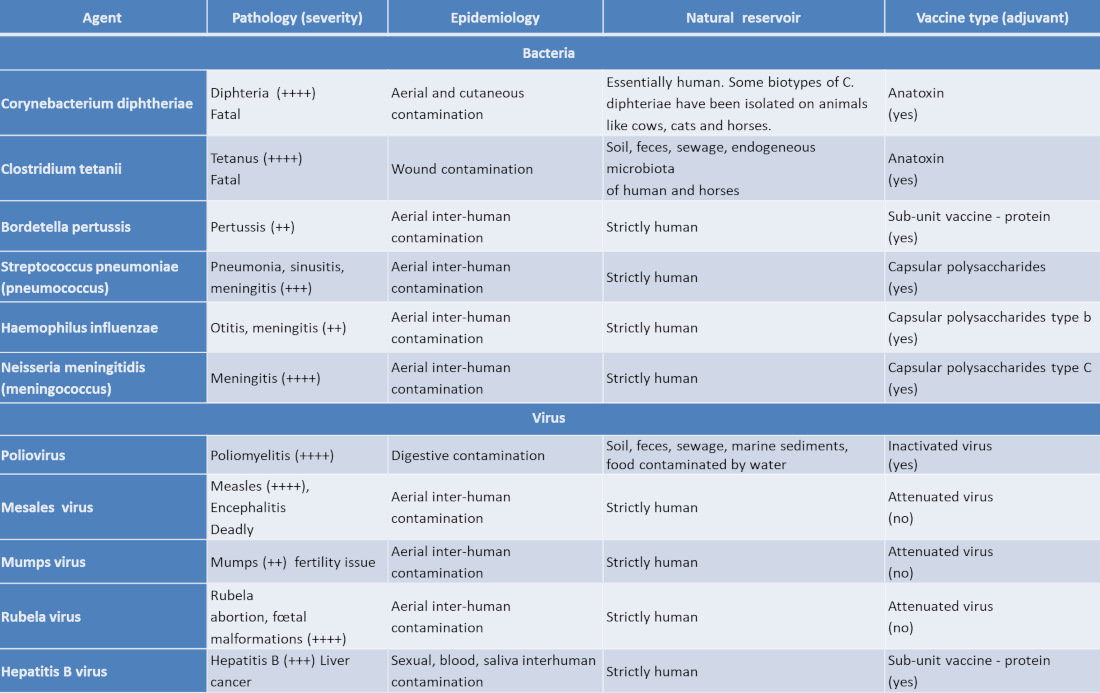
Paradoxically, the disparity between mandatory and recommended vaccines creates in the imagination the idea that recommended vaccines are less important. This is very directly reflected in terms of vaccination coverage. In children, the official calendar recommends 11 vaccines, only 3 of which are mandatory (see Table).
WHO immunization coverage figures comparing European countries are not good for vaccines recommended in France. For example, in 2012, while hepatitis B vaccination coverage for children aged 2 years old was 74% in France, it was more than 86% in Germany and 96% in Belgium and Spain, three countries in which there is no vaccination obligation.
In 2012, the Court of Accounts reported on the cost and effectiveness of vaccination policy in France. This report was followed in 2013 by that of Mr Georges Labazée for the Senate Social Affairs Committee. In 2014, the High Council on Public Health (HCSP) issued an opinion on vaccination policy that called for a debate by the health authorities to decide on vaccination obligations. In 2015, the Minister of Health referred the issue to Senator Sandrine Hurel. Its 2016 report also called for an end to the status quo in this area and for a major consultation on vaccination to determine what collective risks France was prepared to take to remove individual coercion.
This major consultation took place during 2016 under the direction of Professor Alain Fischer. The report submitted to the Minister on 30 November 2016 concluded that the vaccination obligation should be temporarily extended to all the vaccines recommended in the schedule (by adding an exemption clause allowing individual refusal of the vaccine), while retaining in the long term the possibility of completely lifting the obligation once confidence in the vaccines is restored [6].
It is in this vein that the government announced in the summer of 2017 that it had decided in favour of mandatory vaccination for the 11 early childhood vaccines. These are not exactly 11 vaccines, but four vaccine preparations (several vaccines are multivalent) that protect against 11 serious diseases.
References and notes
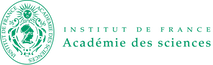
Cover image. Computer generated image representing the tetanus bacillus in the form of persistent spores [Royalty-free]
[1] Moulin A-M. L’aventure de la vaccination. Paris: Fayard; 1996. 498 p. (in french)
[2] Swales JD. The Leicester anti-vaccination movement. Lancet. 1992;340(8826):1019-21
[3] Perrot A, Schwartz M. Pasteur et ses lieutenants: Roux, Yersin et les autres, Odile Jacob; 2013. 270 p. (in french)
[4] Floret D. Les résistances à la vaccination. Med Sci (Paris). 2010;26(12):1087-93
[5] Larson HJ, de Figueiredo A, Xiahong Z, Schulz WS, Verger P, Johnston IG, et al The State of Vaccine Confidence 2016: Global Insights Through a 67-Country Survey. EBioMedicine. 2016;12:295-301
[6] Fischer A. (dir.) Rapport sur la vaccination – Comité d’orientation de la concertation citoyenne sur la vaccination, novembre 2016. Paris Ministère des Affaires sociales et de la Santé ; 2016. 502p. http://www.ladocumentationfrancaise.fr/rapports-publics/164000753/index.shtml (in french)
[7] Launay O, Floret D. Vaccination against Hepatitis B: What’s Up? Rev Prat. 2015;65(7):953-61
[8] Launay O, Floret D. Hepatitis B vaccination: a review. Med Sci (Paris). 2015;31(5):551-8
[9] Gherardi RK, Coquet M, Cherin P, Authier FJ, Laforet P, Belec L, et al. Macrophagic myofasciitis: an emerging entity. Groupe d’Etudes et Recherche sur les Maladies Musculaires Acquises et Dysimmunitaires (GERMMAD) de l’Association Francaise contre les Myopathies (AFM). Lancet. 1998;352(9125):347-52
[10] Gherardi RK. Lessons from macrophagic myofasciitis: towards definition of a vaccine adjuvant-related syndrome. Rev Neurol (Paris). 2003;159(2):162-4
[11] Gherardi RK, Authier FJ. Aluminum inclusion macrophagic myofasciitis: a recently identified condition. Immunol Allergy Clin North Am. 2003;23(4):699-712
[12] Les adjuvants aluminiques : le point en 2016. Académie de pharmacie; 2016 (in french)
[13] Van Der Gucht A, Aoun Sebaiti M, Guedj E, Aouizerate J, Yara S, Gherardi RK, Evangelista E, Chalaye J, Cottereau AS, Verger A, Bachoud-Levi AC, Abulizi M, Itti E, Authier FJ Brain 18F-FDG PET Metabolic Abnormalities in Patients with Long-Lasting Macrophagic Myofascitis J Nucl Med. 2017 Mar;58(3):492-498. doi: 10.2967/jnumed.114.151878. Epub 2016 Oct 20.
[14] Grandjean P, White RF. Effects of methylmercury exposure on neurodevelopment. JAMA. 1999;281(10):896; author reply 7
[15] Thompson WW, Price C, Goodson B, Shay DK, Benson P, Hinrichsen VL, et al. Early thimerosal exposure and neuropsychological outcomes at 7 to 10 years. N Engl J Med. 2007;357(13):1281-92
[16] Hopper E. The River: A Journey to the Source of HIV And AIDS: Lippincott Williams and Wilkins; 1999. 1070 p.
[17] Worobey M, Santiago ML, Keele BF, Ndjango JB, Joy JB, Labama BL, et al. Origin of AIDS: contaminated polio vaccine theory refuted. Nature. 2004;428(6985):820.
[18] Plotkin SA. CHAT oral polio vaccine was not the source of human immunodeficiency virus type 1 group M for humans. Clin Infect Dis. 2001;32(7):1068-84.
[19] Faria NR, Rambaut A, Suchard MA, Baele G, Bedford T, Ward MJ, et al. HIV epidemiology. The early spread and epidemic ignition of HIV-1 in human populations. Science. 2014;346(6205):56-61.
[20] Sansonetti P. Vaccins. Odile Jacob ; 2017. 222 p. (in french)
[21] Gregson AL, Edelman R. Does antigenic overload exist? The role of multiple immunizations in children. Immunol Allergy Clin North Am. 2003;23(4):649-64.
[22] Gomez de Aguero M, Ganal-Vonarburg SC, Fuhrer T, Rupp S, Uchimura Y, Li H, et al The maternal microbiota drives early postnatal innate immune development. Science. 2016;351(6279):1296-302.
[23] van Panhuis WG, Grefenstette J, Jung SY, Chok NS, Cross A, Eng H, et al. Contagious diseases in the United States from 1888 to the present. N Engl J Med. 2013;369(22):2152-8
[24] Georges S, Lepoutre A, Dabernat H, Levy-Bruhl D. Impact of Haemophilus influenzae type b vaccination on the incidence of invasive Haemophilus influenzae disease in France, 15 years after its introduction. Epidemiol Infect. 2013;141(9):1787-96.
[25] Mina MJ, Metcalf CJ, from Swart RL, Osterhaus AD, Grenfell BT. Long-term measles-induced immunomodulation increases overall childhood infectious disease mortality. Science. 2015;348(6235):694-9
[26] Floret D. Measles vaccination. Rev Prat. 2010; 60(10):1368-70.
[27] Antona D, Levy-Bruhl D, Baudon C, Freymuth F, Lamy M, Maine C, et al Measles elimination efforts and 2008-2011 outbreak, France. Emerg Infect Dis. 2013;19(3):357-64.
The Encyclopedia of the Environment by the Association des Encyclopédies de l'Environnement et de l'Énergie (www.a3e.fr), contractually linked to the University of Grenoble Alpes and Grenoble INP, and sponsored by the French Academy of Sciences.
To cite this article: TOURNIER Jean-Nicolas (May 7, 2019), Vaccines, a proven protection against pathogens in our environment, Encyclopedia of the Environment, Accessed April 20, 2024 [online ISSN 2555-0950] url : https://www.encyclopedie-environnement.org/en/health/vaccines-proven-protection-against-pathogens-environment/.
The articles in the Encyclopedia of the Environment are made available under the terms of the Creative Commons BY-NC-SA license, which authorizes reproduction subject to: citing the source, not making commercial use of them, sharing identical initial conditions, reproducing at each reuse or distribution the mention of this Creative Commons BY-NC-SA license.