


Multiple sclerosis and the environment: From the gut to the brain
PDF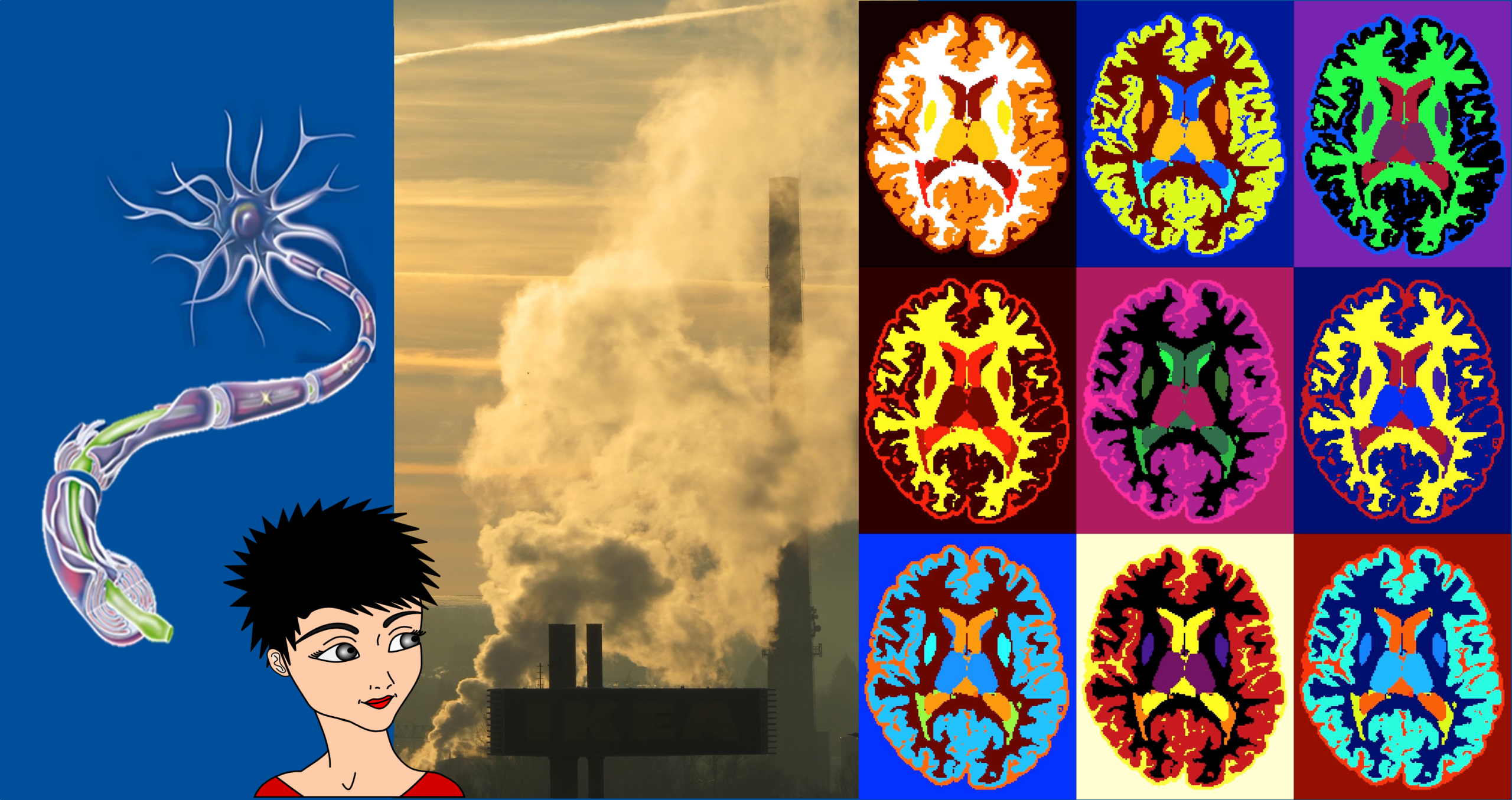
Long considered a perfectly protected organ — notably by the skull and the blood-brain barrier – the brain is in fact not isolated from the rest of the body, or from its environment. It constantly interacts with its surroundings and possesses a great capacity for adaptation and defence against external threats. These interactions are essential to its development and proper functioning. However, certain environmental factors can disrupt this balance. Viral infections, such as those caused by the Epstein-Barr virus (EBV), or a lack of vitamin D—linked, for example, to limited exposure to sunlight—are now considered factors that may influence the risk of developing certain neurological diseases. Multiple sclerosis is a good illustration of this complexity: in this disease, the quality of the environment appears to play a role in both its onset and its progression, by interacting with the brain’s protective mechanisms.
- 1. Multiple sclerosis: a disease of the brain and the immune system
- 2. Who is affected?
- 3. Where genetics and environment intersect
- 4. What, then, is the role of the environment?
- 4.1 Viruses and MS: EBV at the forefront
- 4.2 MS and gut microbiota: the link that could change everything
- 4.3 Vitamin D and MS: the sun as an ally
- 4.4 Diet and obesity
- 4.5 Hormones in the spotlight
- 4.6 Smoking and stress: Two silent contributors to MS
- 4.7 The air we breathe and the risk of MS: an environmental warning
- 4.8 High temperatures, severe symptoms
- 4.9 And what about ‘forever’ pollutants?
- 5. Social determinants of health and lifestyle
- 6. Epigenetics and MS: the environment, the conductor of our gene expression
- 7. Messages to remember
1. Multiple sclerosis: a disease of the brain and the immune system
- The most common form is relapsing-remitting: relapses (sudden worsening of symptoms), followed by partial or complete remission.
- Some cases progress to a secondary progressive form (gradual worsening following more widespread damage to the brain and spinal cord, leading to a disability that worsens over time).
- Others are primary progressive from the outset, with gradual deterioration without distinct relapses.
Diagnosis relies on a medical examination, MRI and analysis of cerebrospinal fluid.
There is currently non cure for MS, but certain medications may reduce the number of relapses, limit the development of new lesions and slow the progression of disability by targeting inflammation.
2. Who is affected?
On average, one person is diagnosed with this condition every five minutes worldwide. The physicians first assess the progression of neurological symptoms (visual disturbances, tingling, numbness, problems with balance and walking, unexplained fatigue). An MRI scan of the brain and spinal cord (see introductory figure) allows typical lesions to be visualized. A lumbar puncture may reveal signs of inflammation of the nervous system. The diagnosis is made after ruling out other diseases with similar symptoms.
2.1 Predominantly affected women

In 2023, MS affects nearly 3 million people worldwide, including 100,000 in France. It mainly affects women [1] (Figure 2), a pattern observed across the globe. Several factors (which are not mutually exclusive) explain this clear imbalance: (i) the role of sex hormones (oestrogen, puberty, pregnancy), (ii) a female immune system that is, on average, more reactive, (iii) epigenetic factors modulated by the environment.
2.2 It is the leading cause of severe disability in young adults, excluding accidents or trauma
Although MS can occur at any age, it primarily affects young adults. Around 1% of cases involve children under the age of 18, but the incidence is highest between the ages of 20 and 54, peaking around 30–35 years (mean age at diagnosis : 32).
A recent study shows this is precisely the age group in which the disease most disrupts professional, social and family life. By 2035, the majority of new cases are expected to continue to occur in this age group, justifying targeted health measures [2].
2.3 It is more common in regions far from the equator
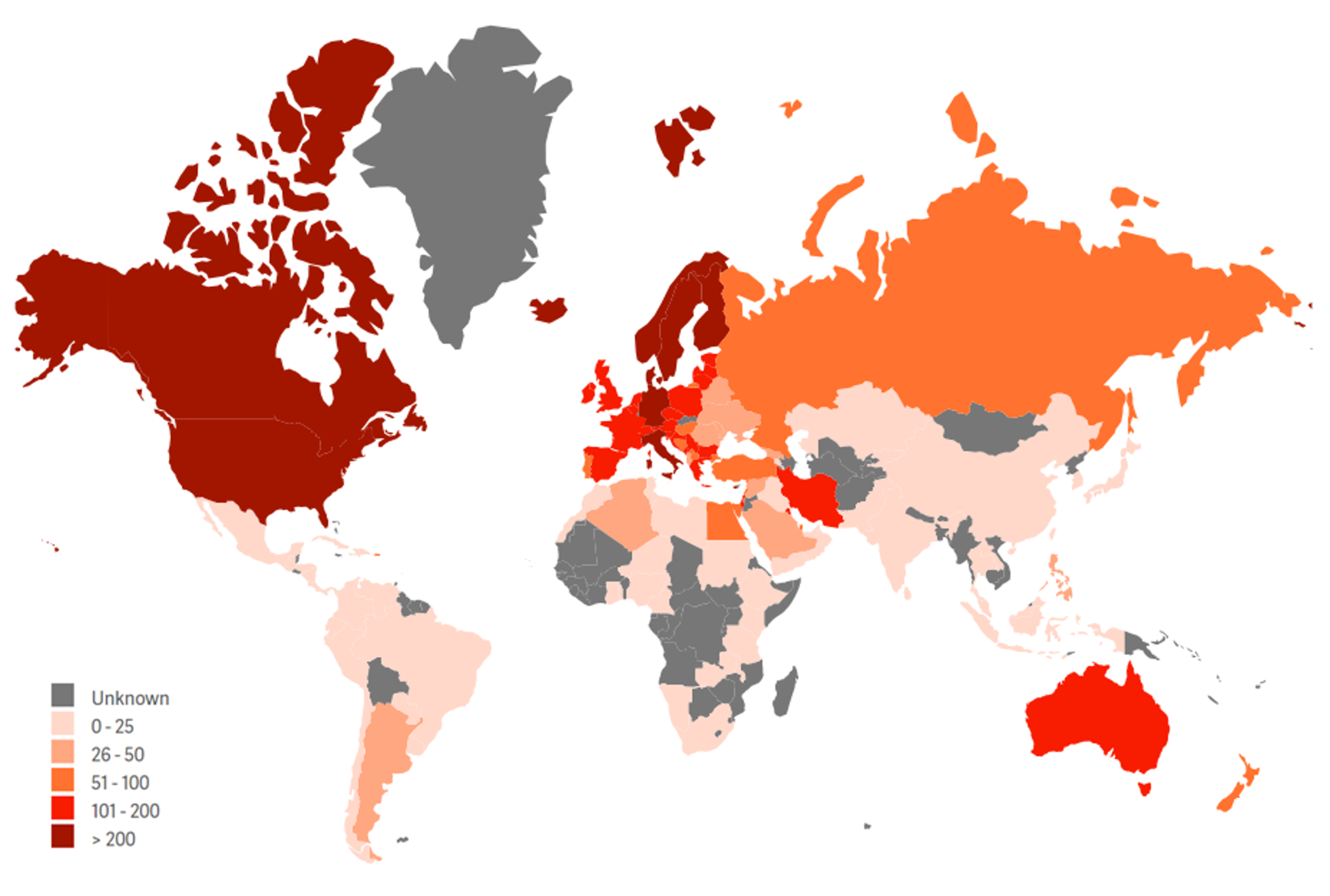
There is a marked north–south gradient: MS is more common at higher latitudes, farther from the equator. This distribution suggests that environmental factors (vitamin D, lifestyle, infections, etc.) play a significant role in interaction with genetic predisposition.
MS is less common among Japanese, Chinese and Native Americans, and more common among Palestinians and Sardinians. In America, it affects Black people more and Hispanics or Asians less (see Chapter 3 below). In France, more aggressive forms are sometimes observed in individuals of African origin.
This trend can be attributed both to improved diagnosis and monitoring (and therefore longer survival), and to an increase in incidence. In France, the prevalence of MS remains higher in the north than in the south of the country (Figure 3).
3. Where genetics and environment intersect
There is There is no single ‘MS gene, but rather a polygenic predisposition. The genetic risk stems from the combination of hundreds of common variants in the genome:
- The strongest genetic factor for MS is the HLA-DRB1*15.01 haplotype located in the HLA (major histocompatibility complex) region on chromosome 6. It facilitates the presentation of myelin or viral antigens to CD4+ T lymphocytes, promotes the breakdown of immune tolerance and demyelination, but only in the presence of other factors (HHV infections, environmental influences and lifestyle)
- Other genetic variants (non-HLA): The disease has a familial component, and over 200 genetic variants increase the risk of MS. Together, they account for approximately 48% of its heritability.
- Genetic factors influencing disease severity (distinct from susceptibility): The HLA-DRB1*15.01 haplotype is strongly associated with the risk of developing MS, but its role in faster progression remains debated. Certain genes involved in neurodegeneration (myelin repair, neuronal survival, inflammatory response) may accelerate the progression to a progressive form. No single gene determines severity, but their combination may favour a more aggressive course.
Genetics alone cannot explain the onset of the disease. Studies of twins show that the risk is not entirely determined by genes. The rapid surge in cases in certain communities, such as the Faroe Islands, is also inconsistent with a strictly genetic origin. MS is therefore not a hereditary disease.
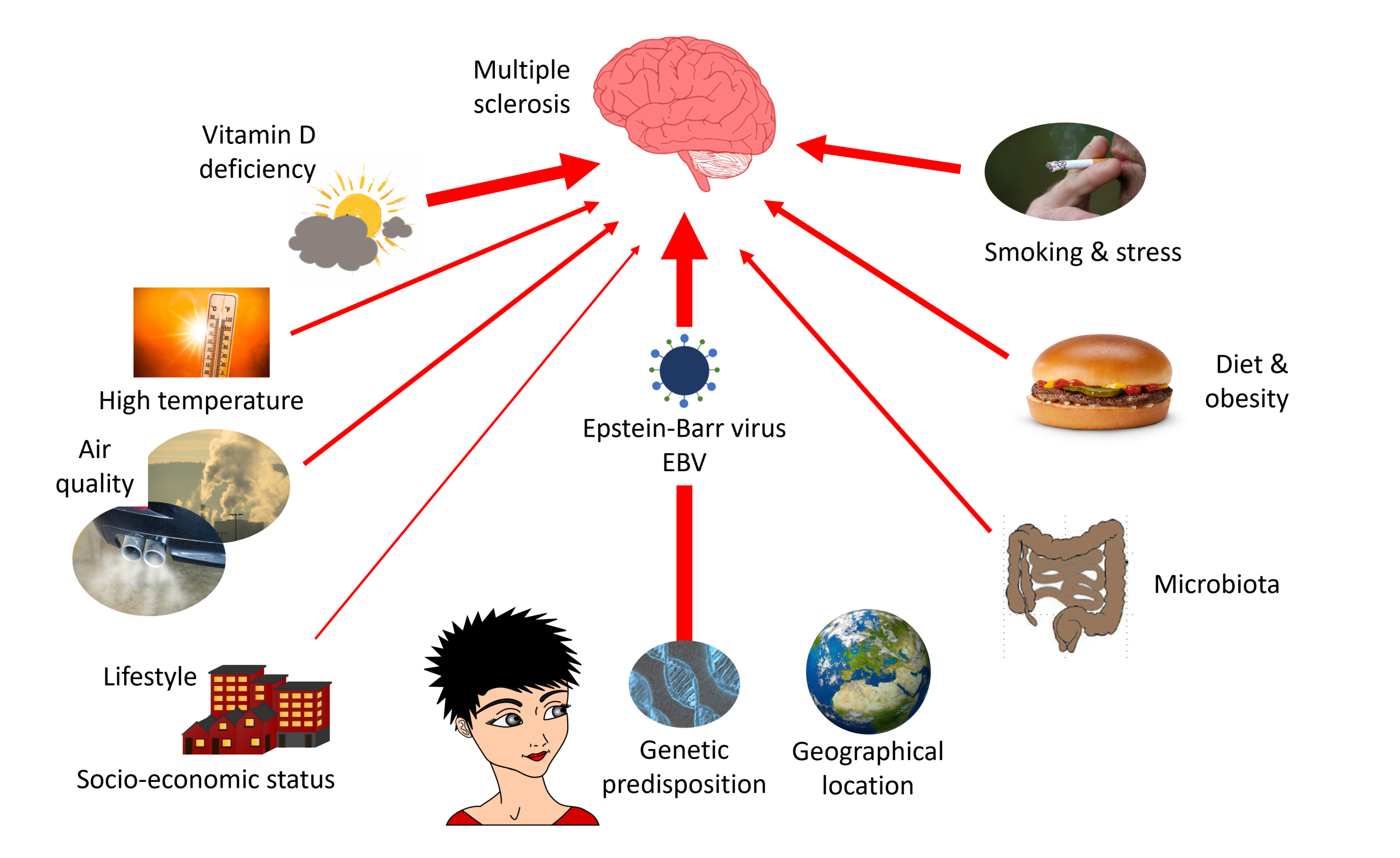
4. What, then, is the role of the environment?
In human health, the environment encompasses all the natural and social factors surrounding an individual (lifestyle, place of residence, socio-cultural context, occupational exposure, infections, etc.). These factors, known as ‘determinants of health’, strongly influence the risk of developing a disease.
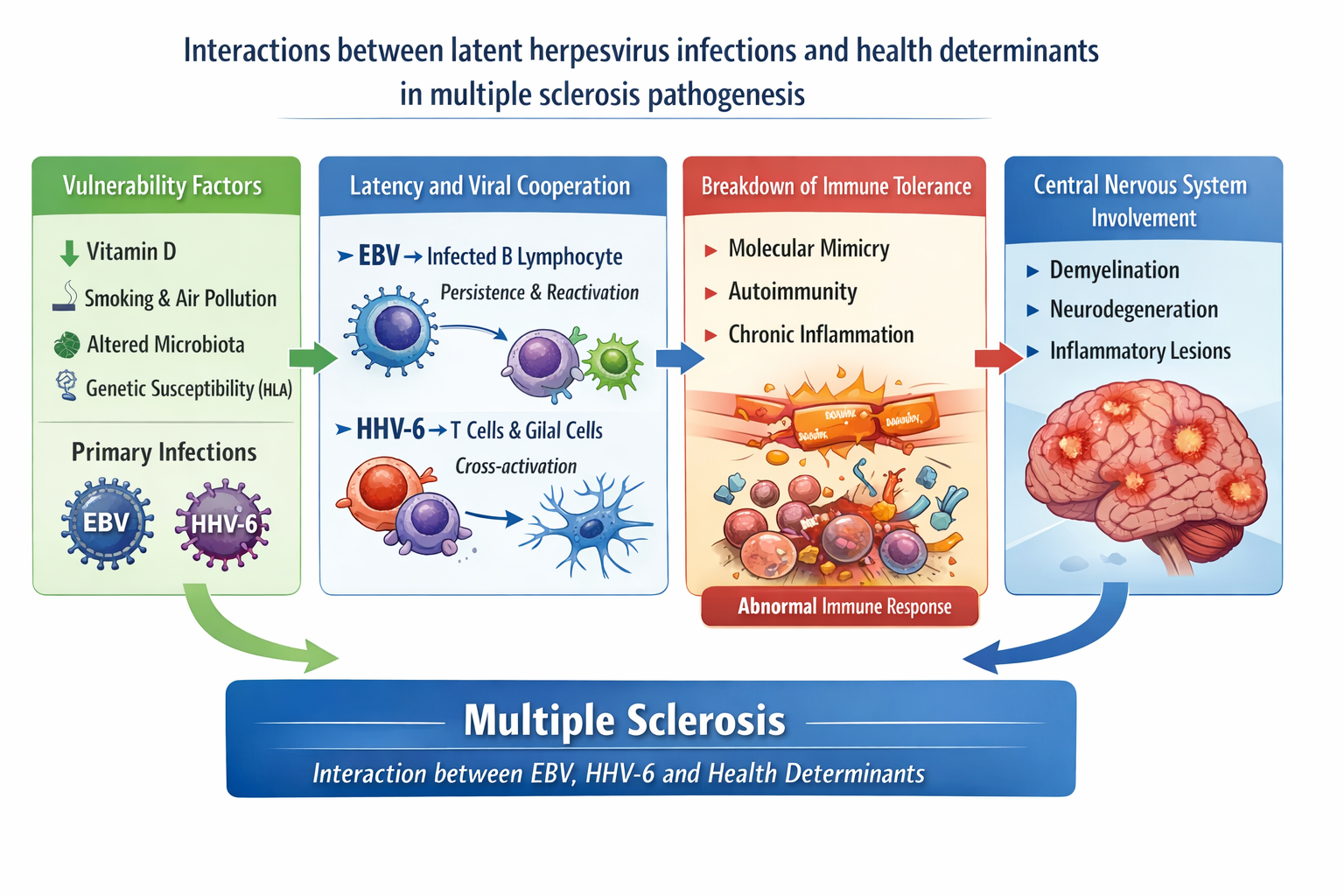
4.1 Viruses and MS: EBV at the forefront
This highly prevalent virus (95–99% of the population infected at some point in their lives) persists in B lymphocytes and induces lasting changes in the immune system. The association between EBV and MS has been known since the 1980s: late-life exposure, often manifesting as infectious mononucleosis almost invariably precedes the disease and significantly increases the risk. People who are EBV-seronegative have an extremely low risk of MS, unlike those who are infected [3].
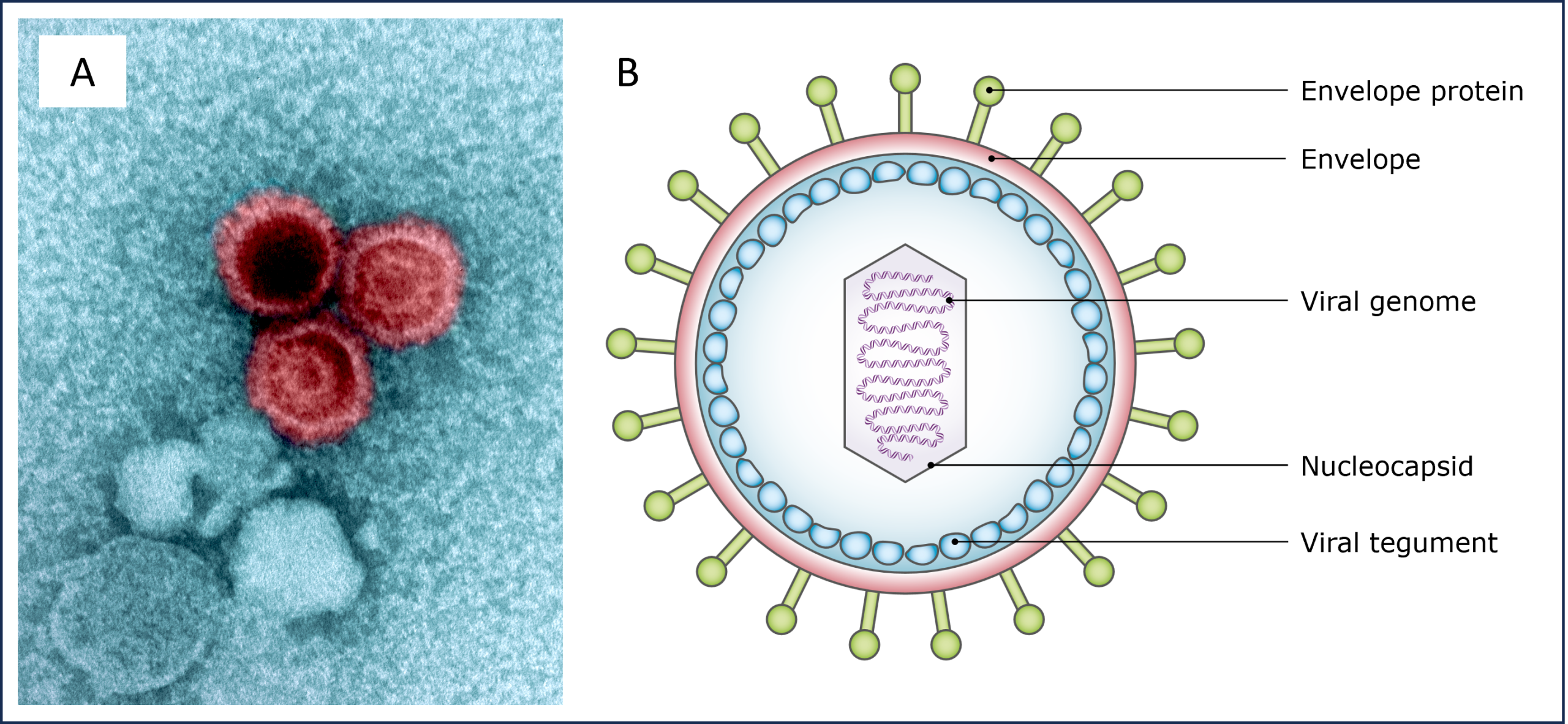
EBV is a herpesvirus (HHV-4) transmitted via saliva. Early infection in childhood is often asymptomatic, whereas late primary infection frequently causes mononucleosis (sore throat + severe fatigue), an intense immune response that appears to promote the MS onset. Conversely, cytomegalovirus (HHV-5) appears to have a neutral or even protective effect.

In 2022, a major study of over 10 million young US military personnel followed for ~20–30 years confirmed this very strong association: EBV infection almost invariably precedes MS (risk increased by ~32-fold after seroconversion) and establishes this virus as the main suspected cause of the disease [4].
The main mechanism cited is molecular mimicry: certain EBV antigens resemble proteins found in oligodendrocytes (myelin-producing cells), triggering an autoimmune attack and the demyelination characteristic of MS. EBV therefore appears to be a key factor, but other herpesviruses (VZV/HHV-3, HHV-6) or respiratory viruses (including SARS-CoV-2) could act as co-determinants, modulating the timing, intensity or location of the autoimmune response. MS would thus result from ‘chronic viral dysbiosis’ combined with other risk factors.
In conclusion, the immune response to EBV constitutes a key causal factor in the aetiology of MS, going far beyond a simple correlation [5]. This paves the way for new therapeutic strategies: antivirals, immunotherapies targeting EBV and associated herpesviruses, and, above all, the development of an anti-EBV vaccine to prevent or mitigate the severity of the infection and, consequently, reduce the risk or severity of MS (Figure 5).
4.2 MS and gut microbiota: the link that could change everything

The brain and the microbiota communicate in particular via the vagus nerve and through the bloodstream: metabolites produced by the bacteria in the microbiota enter the bloodstream and directly influence cognition, behaviour and brain physiology. This microbiota-gut-brain axis is implicated in numerous conditions, including neurodegenerative, psychiatric and cardiovascular diseases (Figure 6).
In mice, animals raised under sterile conditions exhibit a milder form of the disease. The same is true for mice genetically predisposed to developing MS-like symptoms. This protective effect is reversible: colonisation of their intestines by a normal microbiota in adulthood restores susceptibility to the disease. Faecal transplants confirm this role. Thus, when microbiota from one of a pair of twins, only one of whom has MS, is transferred to healthy mice, those receiving the microbiota from the affected twin develop the disease, whereas those receiving the microbiota from the healthy twin remain unaffected. These results suggest that the microbiota is necessary for the onset of MS, depending on immune and inflammatory mechanisms (Figure 7) [6].

4.3 Vitamin D and MS: the sun as an ally
Exposure to sunlight helps the body produce vitamin D, which may protect against multiple sclerosis (MS). This explains why MS is more common in the north than in the south of France. In the United States, 200,000 women taking 400 IU of vitamin D saw their risk of MS reduced by 40%, and among 7 million military personnel, a blood level of at least 100 nmol/L was associated with a 51% reduction in risk [7]. The risk is also influenced by genetics [8] and the time of birth [9]: children born in May or whose mothers were deficient in vitamin D early in pregnancy are at higher risk. Today, vitamin D supplementation is recommended for patients with MS.
4.4 Diet and obesity
Obesity, which is rising sharply worldwide, results from an unbalanced diet, increased sedentary lifestyles, insufficient sleep and exposure to pollutants (including endocrine disruptors) (Figure 8). It stimulates the production of pro-inflammatory hormones (particularly leptin) and increases the risk of developing MS, especially in obese children and adolescents [10].
In adults, it exacerbates disability without increasing the number of relapses or lesions visible on MRI. Furthermore, a high salt intake exacerbates inflammation and disease activity. Sugary drinks worsen symptoms and disability, whilst beer appears to be the type of alcohol most strongly associated with the risk of MS.
4.5 Hormones in the spotlight
Sex hormones influence the risk of multiple sclerosis. Before puberty, the risk is similar in boys and girls. Afterwards, women are significantly more affected. Early puberty, particularly when associated with obesity, increases this risk. The premenstrual period often triggers relapses, whereas oral contraception does not exacerbate the condition. According to the PRIMS study, the number of relapses decreases during pregnancy (particularly in the third trimester), but a rebound frequently occurs within three months of giving birth.
Sex hormones affect the immune system and the myelination of the nervous system. Endocrine disruptors (See Endocrine disruptors and human health), (chemical or natural substances that interfere with the hormonal system), may therefore play a role in the onset or worsening of MS.
4.6 Smoking and stress: Two silent contributors to MS
Smoking (active or passive) is a well-established risk factor for multiple sclerosis. This risk increases with the duration and intensity of exposure. Exposure to tobacco during childhood (parental smoking) also increases this risk.
Beyond triggering the disease, smoking worsens its progression: it accelerates the progression to more severe forms, increases damage to the central nervous system and promotes brain atrophy visible on MRI scans [11].
Finally, the risk becomes extremely high (up to 30 times greater) when smoking is combined with a genetic predisposition and exposure to organic solvents (paints, varnishes or paint strippers, etc.) [12].
Stress has long been suspected of contributing to the onset or progression of multiple sclerosis. Several studies show a clear link between stressful events and an increased risk of MS relapses, suggesting that psychological stress exacerbates inflammation and increases the frequency of relapses [13] (See Acute stress, chronic stress, stress management methods in humans).
4.7 The air we breathe and the risk of MS: an environmental warning
Air pollution from gases (NO₂, NOx, O₃, CO, SO₂, volatile organic compounds – VOCs) and fine or ultrafine particles (PM2.5 and PM10), of natural or anthropogenic origin (See Airborne particulate matter and their health effects). The finest particles (PM2.5) can reach the brain directly, either by crossing the blood-brain barrier or via the nasal route through the olfactory bulb. They then trigger cerebral inflammation, activate microglia, generate oxidative stress, impair the vascular endothelium and lead to the accumulation of proteins implicated in neurodegenerative diseases (Figure 8).
There is now a well-documented link between air pollution (PM2.5 – NO₂ – O₃) and multiple sclerosis (MS), both in terms of the onset of the disease and the occurrence of relapses. Several international studies have shown an association between exposure to PM2.5, SO₂, CO (and sometimes lead) and the onset of MS, including in children [14]. A few examples:
- In Tehran, the incidence of MS is significantly higher in the most polluted neighbourhoods (PM₁₀, SO₂, NO₂, NOx), and PM₁₀ levels correlate with the number of relapses observed in the same month and the following month [15].
- In Lombardy, a dose-dependent relationship has been established between exposure to PM₁₀ during the preceding seven days and the risk of hospitalization for an MS relapse [16].
- Research conducted in Strasbourg has highlighted a link between PM10 levels in the three days preceding the symptom onset and relapses, particularly during cold weather.
- A study from the Île-de-France region published in 2021 showed that PM2.5 plays a particularly significant role in triggering relapses in young adults under the age of 30 [17].
Overall, the main mechanism involves a systemic pro-inflammatory state induced by fine particulate matter, which not only exacerbates MS but also increases the risk of other vascular complications such as myocardial infarction or ischaemic stroke.
4.8 High temperatures, severe symptoms
Climate change, one of the greatest current threats to public health (See Climate change: what effects on our health?), could also influence the progression of certain neurological diseases, particularly MS (Figure 8).
For many individuals with mild MS, the heat is not just uncomfortable: it becomes a real limiting factor in daily life.
4.9 And what about ‘forever’ pollutants?
PFAS (per- and polyfluoroalkyl substances found in a wide range of products: non-stick coatings, waterproof textiles, fire-retardant foams, food packaging, …) and OH-PCBs or hydroxy-polychlorinated biphenyls (industrial fluids) are persistent organic pollutants, known to contribute to the onset and progression of autoimmune diseases, including effects potentially mediated by gene-environment interactions. A recent Swedish study shows statistically significant associations, but these results do not prove that PFAS or OH-PCBs directly cause MS [20].
5. Social determinants of health and lifestyle
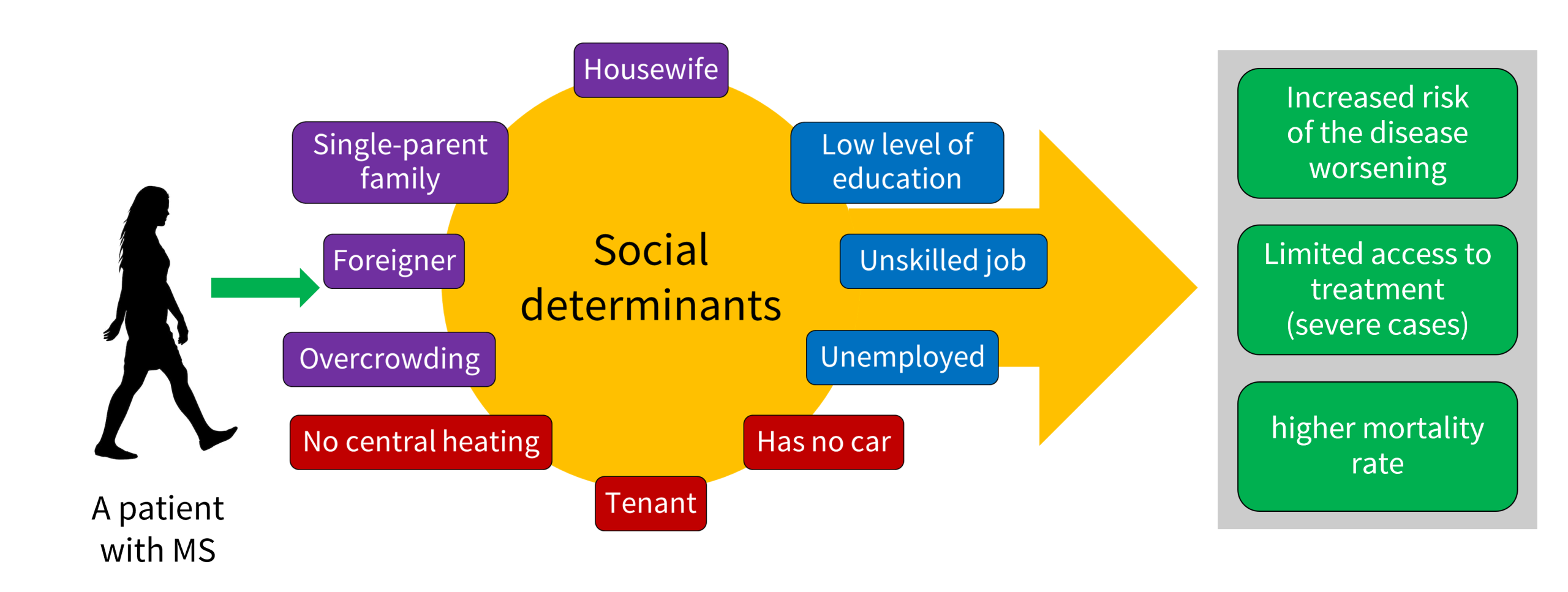
These health determinants appear to play a role in MS, as in other autoimmune diseases. For example, improved hygiene, while essential, is paradoxically accompanied by an increased risk of autoimmune diseases and allergies. According to the hygiene hypothesis, early exposure to certain infectious agents (bacteria, viruses, parasites) confers immune protection, whereas a later encounter with these same agents can trigger pathological auto e reactions. Several studies support the idea of a strong environmental influence:
- A large-scale study of 30,000 Canadian families demonstrated the importance of the intrauterine environment and a rapid increase in the sex ratio (more women affected) from the 1970s onwards, a change too rapid to be solely genetic [21].
- Among migrants, the age at which they are exposed to the new environment is decisive: before the age of 15, the individual assumes the risk profile of the host region; after the age of 15, they largely retain the risk profile of their country of origin, especially if they maintain their lifestyle habits.
- A study of migration between the Caribbean and mainland France (conducted in the 1980s) reveals that Caribbean people who remained in the region are less likely to develop MS than those who left before the age of 15, suggesting a protective effect of childhood parasitic infections [22]. Conversely, adults who return to the Caribbean are at increased risk. The recent increase in MS in the region coincides with urbanisation, lifestyle changes and the eradication of parasites. Finally, MS patients infected with certain parasites (e.g. pinworms) experience fewer relapses, a slower progression of disability and fewer lesions on MRI scans than those who are not infected.
5.2 Multiple sclerosis and living conditions: the impact of socio-economic status
6. Epigenetics and MS: the environment, the conductor of our gene expression
Our genes do not express themselves in isolation: the environment strongly regulates them via epigenetic mechanisms (e.g. DNA methylation), without ever altering the DNA sequence itself (See Epigenetics: How the environment influences our genes). These mechanisms, which are highly sensitive to lifestyle and external exposures, likely play a key role in multiple sclerosis (Figure 10). Two major avenues of research are emerging:
- Human endogenous retroviruses (HERVs) [24]
These ancient viral remnants, which have been integrated into our genome for millions of years, are generally silenced by methylation. In some people with MS, they are reactivated (particularly HERV-W) through targeted demethylation, under the influence of environmental and infectious factors. Studies show (i) overexpression of HERV-W, particularly those of the HERV-W group, in the blood, brain and cerebrospinal fluid; (ii) the production of pro-inflammatory molecules that stimulate the immune system; (iii) genetic variants close to these retroviral sequences associated with an increased risk of MS.
- Epigenetic reprogramming of immune cells
The environment (EBV, sunlight, vitamin D) and genetics converge to establish a sustained pro-autoimmune state via measurable epigenetic modifications (particularly in T and B lymphocytes) [25]. The ‘methylation signatures’ observed are statistically linked to: (i) the intensity of the anti-EBV response, (ii) vitamin D status, (iii) cumulative sun exposure, (iv) the risk-associated HLA genotype (e.g. HLA-DRB1*15:01).
These environmental factors thus leave a stable biological imprint in immune cells, promoting the onset and chronicity of the disease.
7. Messages to remember
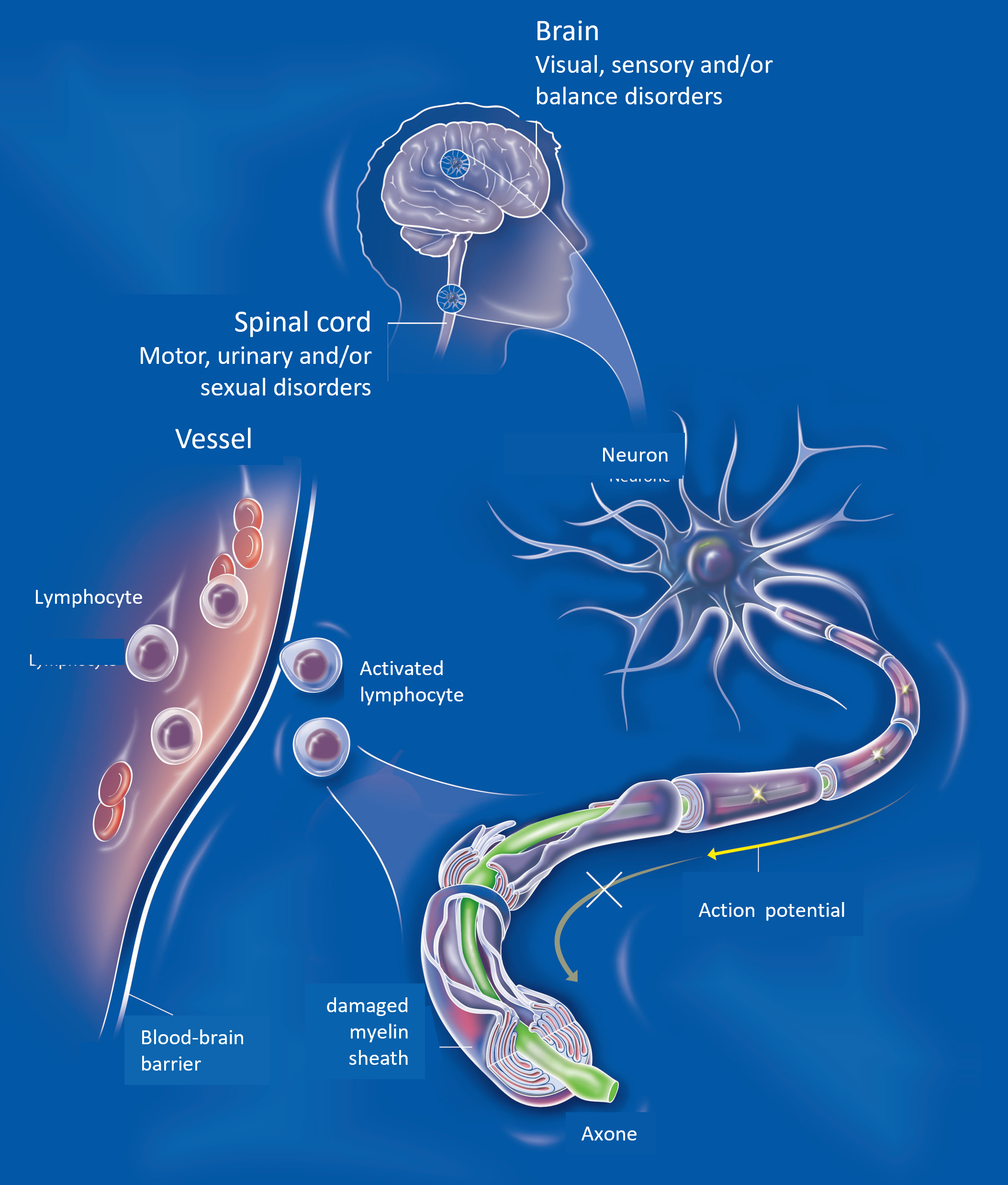
- Multiple sclerosis is a chronic autoimmune disease of the central nervous system, in which the immune system mistakenly attacks myelin, the protective sheath around nerves, causing lesions (plaques) that disrupt nerve transmission.
- MS is a complex disease, influenced by genetic and environmental factors (including lifestyle).
- Epstein-Barr virus (EBV) infection is the most powerful and best-documented environmental factor. An EBV infection (often in the form of infectious mononucleosis) is considered necessary but not sufficient for the development of MS in genetically predisposed individuals. The risk increases significantly following mononucleosis.
- Low vitamin D levels (linked to insufficient sunlight/UVB exposure) significantly increase the risk of developing the disease and also accelerate its progression.
- Smoking increases the risk of triggering MS and clearly accelerates the progression of the disease. Giving up smoking is one of the most important modifiable measures.
- Obesity and being overweight are significant factors, particularly during adolescence. The effect appears to be linked to chronic inflammation and, in all likelihood, to the gut microbiota.
- An imbalance in the gut microbiota is observed in people with MS. It is not yet known whether this is a cause or a consequence.
- Apart from EBV, other viral infections in childhood may play a modulatory role (protection or risk depending on the type and timing), but no other virus has reached the level of evidence seen with EBV.
- Pollutants and persistent chemicals appear to pose an increased risk of MS. Organic solvents and certain air pollutants are also suspected (though evidence is still limited).
- There is almost never a single factor responsible. The most unfavourable combination (e.g. vitamin D deficiency + smoking + EBV + adolescent obesity) greatly increases the risk. Conversely, addressing certain modifiable factors (vitamin D, stopping smoking, maintaining a healthy weight) can reduce the risk and slow progression.
Notes & references
Cover image. Multiple sclerosis and the environment [EEnv montage]. Left: Diseased neuron, see Figure 1 [Diagram source © Inserm, C. Fumat, reproduced with the author’s permission – centre: Pollution [Photo source © Hans via Pixabay] – right: Brain MRI showing MS [Source Credit: © Ilena George and Daniel Reich, National Institute of Neurological Disorders and Stroke, National Institutes of Health, public domain, via Flickr]
[1] Khan, G., Hashim, M.J., 2025. Epidemiology of Multiple Sclerosis: Global, Regional, National and Sub-National-Level Estimates and Future Projections. J Epidemiol Glob Health 15, 21. https://doi.org/10.1007/s44197-025-00353-6
[2] Wang L-y, Wang W-f, Hui S-y, Yang L, Liu Y-x and Li H-j (2025) Emerging epidemiological trends of multiple sclerosis among adults aged 20–54 years, 1990–2021, with projections to 2035: a systematic analysis for the Global Burden of Disease Study 2021. Front. Neurol. 16:1616245. doi: 10.3389/fneur.2025.1616245
[3] Soldan SS, Lieberman PM (2023). Epstein-Barr virus and multiple sclerosis. Nat Rev Microbiol. doi: 10.1038/s41579-022-00770-5.
[4] K. Bjornevik et al., (2022) ‘Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis’, Science, vol. 375, no. 6578, pp. 296–301, Jan. 2022, doi: 10.1126/science.abj8222
[5] Läderach, F.; Münz, C. Altered Immune Response to the Epstein–Barr Virus as a Prerequisite for Multiple Sclerosis. Cells 2022, 11, 2757. https://doi.org/10.3390/cells11172757
[6] S. Trott and I. L. King, ‘An introduction to the microbiome and MS’, Mult. Scler. Houndmills Basingstoke Engl., vol. 24, no. 1, pp. 53–57, Jan. 2018, doi: 10.1177/1352458517737391
[7] K. L. Munger, L. I. Levin, B. W. Hollis, N. S. Howard, and A. Ascherio, ‘Serum 25-hydroxyvitamin D levels and risk of multiple sclerosis’, JAMA, vol. 296, no. 23, pp. 2832–2838, Dec. 2006, doi: 10.1001/jama.296.23.2832
[8] L. E. Mokry et al., ‘Vitamin D and Risk of Multiple Sclerosis: A Mendelian Randomization Study’, PLOS Med., vol. 12, no. 8, p. e1001866, Aug. 2015, doi: 10.1371/journal.pmed.1001866.
[9] C. J. Willer, D. A. Dyment, A. D. Sadovnick, P. M. Rothwell, T. J. Murray, and G. C. Ebers, ‘Timing of birth and risk of multiple sclerosis: population-based study’, BMJ, vol. 330, no. 7483, p. 120, Jan. 2005, doi: 10.1136/bmj.38301.686030.63.
[10] M. A. Gianfrancesco and L. F. Barcellos, ‘Obesity and Multiple Sclerosis Susceptibility: A Review’, J. Neurol. Neuromedicine, vol. 1, no. 7, pp. 1–5, 2016. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5156319/
[11] A. K. Hedström, ‘Smoking and disability progression in multiple sclerosis’, Expert Rev. Neurother., vol. 20, no. 8, pp. 739–741, August 2020, doi: 10.1080/14737175.2020.1743176.
[12] A. K. Hedström, O. Hössjer, M. Katsoulis, I. Kockum, T. Olsson, and L. Alfredsson, ‘Organic solvents and MS susceptibility: Interaction with MS risk HLA genes’, Neurology, vol. 91, no. 5, pp. e455–e462, July 2018, doi: 10.1212/WNL.0000000000005906.
[13] von Drathen S et al. Stress and Multiple Sclerosis – Systematic review and meta-analysis of the association with disease onset, relapse risk and disability progression. Brain Behav Immun. 2024 120:620-629. doi: 10.1016/j.bbi.2024.06.004. Epub 19 June 2024. PMID: 38906489.
[14] A. M. Lavery et al., ‘Urban air quality and associations with paediatric multiple sclerosis’, Ann. Clin. Transl. Neurol., vol. 5, no. 10, pp. 1146–1153, Oct. 2018, doi: 10.1002/acn3.616.
[15] P. Heydarpour, H. Amini, S. Khoshkish, H. Seidkhani, M. A. Sahraian, and M. Yunesian, ‘Potential Impact of Air Pollution on Multiple Sclerosis in Tehran, Iran’, Neuroepidemiology, vol. 43, no. 3–4, pp. 233–238, Dec. 2014, doi: 10.1159/000368553
[16] L. Angelici et al., ‘Effects of particulate matter exposure on multiple sclerosis hospital admission in Lombardy region, Italy’, Environ. Res., vol. 145, pp. 68–73, Feb. 2016, doi: 10.1016/j.envres.2015.11.017.
[17] Januel E et al. Fine Particulate Matter Related to Multiple Sclerosis Relapse in Young Patients. Front Neurol. 21 May 2021;12:651084. doi: 10.3389/fneur.2021.651084. PMID: 34093398; PMCID: PMC8176031.
[18] J. F. Sumowski and V. M. Leavitt, ‘Body Temperature Is Elevated and Linked to Fatigue in Relapsing-Remitting Multiple Sclerosis, Even Without Heat Exposure’, Arch. Phys. Med. Rehabil., vol. 95, no. 7, pp. 1298–1302, July 2014, doi: 10.1016/j.apmr.2014.02.004.
[19] H. Elser et al., ‘Anomalously warm weather and acute care visits in patients with multiple sclerosis: A retrospective study of privately insured individuals in the US’, PLoS Med., vol. 18, no. 4, p. e1003580, Apr. 2021, doi: 10.1371/journal.pmed.1003580
[20] Vaivade A et al. Co-exposure to PFAS and hydroxylated PCBs is associated with increased odds of multiple sclerosis. Environ Int. 2026 Jan;207:109993. doi: 10.1016/j.envint.2025.109993. Epub 11 Dec 2025. PMID: 41411973.
[21] D. Sadovnick, ‘The place of environmental factors in multiple sclerosis: Genes, environment and the interactions thereof in the aetiology of multiple sclerosis’, Rev. Neurol. (Paris), vol. 175, no. 10, pp. 593–596, Dec. 2019, doi: 10.1016/j.neurol.2019.08.003.
[22] P. Cabre et al., ‘Role of return migration in the emergence of multiple sclerosis in the French West Indies’, Brain, vol. 128, no. 12, pp. 2899–2910, Dec. 2005, doi: 10.1093/brain/awh624.
[23] Alfredsson L et al. Observed associations between indicators of socioeconomic status and risk of multiple sclerosis in Sweden are explained by a few lifestyle-related factors. Eur J Neurol. 2023 Apr;30(4):1001-1013. doi: 10.1111/ene.15705. Epub 2023 Feb 8. PMID: 36692896
[24] Morris, G., Maes, M., Murdjeva, M. et al. Do Human Endogenous Retroviruses Contribute to Multiple Sclerosis, and if So, How?. Mol Neurobiol 56, 2590–2605 (2019). https://doi.org/10.1007/s12035-018-1255-x
[25] Simpson-Yap S et al. Epstein-Barr Virus, Lower Vitamin D, Low Sun Exposure, and HLA-DRB1*1501 Risk Variant Share Common Epigenetic Pathways Leading to Multiple Sclerosis Onset. Ann Neurol. 2026 Feb;99(2):341-355. doi: 10.1002/ana.78043. Epub 10 Oct 2025. PMID: 41070760; PMCID: PMC12894492.
The Encyclopedia of the Environment by the Association des Encyclopédies de l'Environnement et de l'Énergie (www.a3e.fr), contractually linked to the University of Grenoble Alpes and Grenoble INP, and sponsored by the French Academy of Sciences.
To cite this article: HOMEYER Pascale (March 23, 2026), Multiple sclerosis and the environment: From the gut to the brain, Encyclopedia of the Environment, Accessed March 28, 2026 [online ISSN 2555-0950] url : https://www.encyclopedie-environnement.org/en/health/multiple-sclerosis-environment-gut-brain/.
The articles in the Encyclopedia of the Environment are made available under the terms of the Creative Commons BY-NC-SA license, which authorizes reproduction subject to: citing the source, not making commercial use of them, sharing identical initial conditions, reproducing at each reuse or distribution the mention of this Creative Commons BY-NC-SA license.


