疫苗,防御病原体的有效措施
疫苗的有效性越来越让人质疑,本文就此进行了一系列反思。疫苗是人类历史上最伟大的科学发现之一,如今在发达国家却饱受争议。但纵观历史,“预防性”接种仍然是人类控制众多传染病的不可或缺的手段。人类是某些病毒的唯一宿主(如乙型肝炎、麻疹、细菌性脑膜炎),其他病原体则源自环境,如破伤风病原体(见上图)源自被粪便污染的土壤、小儿麻痹症病原体则源自被污染的水或食物。甚至像流感这样常见疾病,也可能来源于环境 (如人类流感来自禽流感和猪流感)。本文首先追溯了人类反对和抵制疫苗接种的历史,这段历史始于19世纪的英国,有关疫苗接种的系列公共卫生法规颁布后,遭到了英国人民的强烈反对。
随后,本文对目前出现的有关疫苗的相关争议进行了分析 。在本文最后,文章最后阐述了疫苗接种率下滑将会带来的后果,并探讨了如何平衡强制接种和推荐接种之间的关系。
2014年11月的某个早上,巴基斯坦某省的4名疫苗接种医生遇害。他们被冠以 “传播非伊斯兰疫苗”的罪名,死在了塔利班冲锋枪的子弹下 。为了实施世界卫生组织提出的根除脊髓灰质炎 计划,这一批接种人员不久前才乘车来到巴基斯坦的边境小村庄。在村庄里,医护人员挨家挨户敲门,劝说母亲给孩子们接种骨髓灰质炎的疫苗。目前,只有三个国家仍有小儿麻痹症在人群中传播,巴基斯坦是其中之一。还有一个是尼日利亚,这个国家也发生过疫苗接种人员遇害事件。(还有一个是尼日利亚,而在尼日利亚同样也发生疫苗接种人员被谋杀的事件)。在全球所有小儿麻痹症病例中,来自巴基斯坦的病例占了85%。小儿麻痹症是一种病毒性疾病,可导致肌肉麻痹,患者甚至会因呼吸麻痹而死亡。 多种疫苗可以预防小儿麻痹症,可以有效守护每一位儿童的健康。
这一充满了极端和暴力的血腥事件,便是 疫苗自其诞生以来受到反抗的缩影。在疫苗问世的短暂历史中,这些来到巴基斯坦的接种人员并不是第一批被蒙昧主义祸害的受害者,疫苗接种从问世就引起了不少冲突和抵抗。不是所有的反抗都是激进或毫无根据的,它们的根源都是相似的社会问题。
反对疫苗接种,最终的受害者始终是儿童,比如2008年至2012年期间麻疹在法国卷土重来,导致10人死亡,确诊病例达到23000人, 5000多名患儿因并发症而住院。同时,2012年以来,法国还报告了3例严重的破伤风病例。 2015年6月,图尔的一名8岁儿童被紧急送往医院,起因是被陶瓷碎片划伤后得了破伤风。这本是不应该发生的,而男孩却因此在重症监护室呆了整整三周。此前,儿科医生曾征得男孩父母的同意为其伪造了一份疫苗接种证明。这名医生因此被医师协会除名并取消其行医资格。
本文首先回顾了反对接种疫苗的历史,然后分析了其产生的原因,并在最后讨论了如何在强制接种和自愿接种之间达到平衡。
1. 抵制疫苗接种:历史遗留问题
1.1. 遭遇嘲讽的第一支疫苗

抵制疫苗的运动从疫苗诞生的那一天就开始了。1796年,爱德华·詹纳(Edward Jenner,1749-1823)发明的第一支天花疫苗就遭受了公众的抵制。 1802年,英国漫画家创作的漫画对天花疫苗的安全性提出了质疑,画中的人们因为接种了牛痘而变成牛和猪(图 1)。
天花是一种爆发性的病毒传染病,早在古埃及就已经出现(发现木乃伊身上有天花痘痕)。肆虐千年的天花在社会各个阶层中蔓延开来(路易十五在小特里亚农因感染天花而亡),引发了可怕的流行病传播。天花导致半数患者死亡,幸存者身上也会留下恐怖的疤痕。直到 20世纪中叶,每年仍有5000万人感染天花,其中200万人死亡[1]。
即使这样,当疫苗作为公共卫生防御措施出现时,嘲讽竟然演化为公然的反对甚至是血腥的反抗。在第一部强制接种疫苗的法案起草时便已出现了反抗,从侧面反映了当时社会的动荡局势以及义务、国家权威和个人自由之间的复杂关系。
1.2. 起源:英国医生詹纳推广牛痘疫苗
英国——爱德华·詹纳的家乡,是世界上第一个实行强制性疫苗接种的国家(1853年)。法律强制要求儿童接种疫苗,否则父母将面临高额罚款或监禁。当时的英国一穷二白,卫生系统尚未设立,流行病学监测屈指可数,疫苗接种率并不足以减少疾病传播。当时的英国贫富差距非常大,而没有接种疫苗的人往往是穷人。
由于法律的局限性,1867年政府将接种儿童的年龄扩展到14岁以下。疫苗接种人员通过走访每个家庭来核实出生记录上的儿童是否接种了疫苗。1871年,该法案得到了进一步完善,接种人员必须送达与儿童出生证明登记相符的疫苗接种证明。尽管对于国家来说维护该系统需要投入大量资金,但实施后的效果明显。不久,民众越来越不能容忍国家干涉个人事务。这些法律被认为是对个人自由的妨碍。
1876年,在约克郡的基斯利,疫苗接种员曾被暴徒逮捕并短暂关押。从此,反疫苗的联盟成立。1886年,莱斯特超过 6000人因未接种疫苗而被起诉。但随后2万多人的示威游行导致诉讼终止,莱斯特地区成为英国抵制疫苗的先锋[2]。在暴乱的影响下, 1895年英国政府在立法上妥协,疫苗接种变为“良心条款”,法律允许公民拒绝接种疫苗。
[来源:©James Gathany内容提供者:CDC,维基百科]
最初,这一法令受到极大限制,因为需要两名法官签字才能通过和施行。在某些法官认同疫苗接种的地区,法令不可能实施。而 1907年,在民众的压力下,法令变得更加灵活,只需要签字声明即可。1948年,在拥护和抵制疫苗的近百年斗争之后,英国领先于许多国家率先废除了对天花疫苗的强制性接种政策。值得一提的是,在法国, 1904年建立的天花疫苗强制性政策一直持续到 1980年(天花根除之年)。
1.3. 全球抵制接种
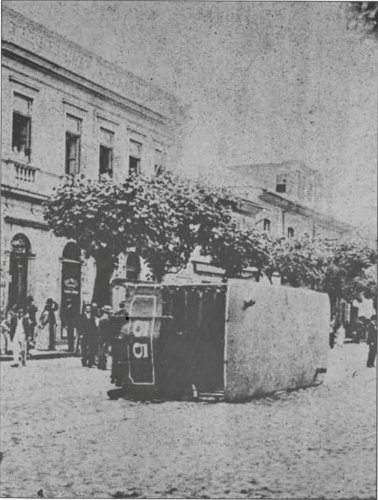
[来源:巴西某周刊,发表于1904年11月27日,维基百科]
英国并不是当时唯一遭遇疫苗接种反抗的国家。1904年,巴西发生了一场抵制天花疫苗接种的暴动。这场动乱被称为“牛痘起义”(图 3)。当时,黄热病和天花正在里约热内卢的贫民区肆虐。1904年10月31日,巴西国会通过了一项法令,强制人们接种天花疫苗。法令允许管制员强行进入家庭。这种对个人自由的干涉导致了人民奋起反抗。反对派成立了“反疫苗联盟”。连续 6天,整个里约热内卢因道路障碍和抢劫而瘫痪。等到暴乱被平息后,已有接近30人死亡,110人受伤。在美国,反疫苗联盟也发展起来。与英国一样,在美国大多数州都采用“良心条款”。
1.4. 一个特例——法国
在反抗疫苗接种的历史上,法国算得上是一个特例。在 19世纪和 20世纪初,疫苗并未遭到大规模的反对。这里可能有几个原因:首先,与“现代疫苗之父”路易·巴斯德(Louis Pasteur,1822-1895)对整个法国的影响有很重要的关系。因为对法国战胜疾病和疾病带来的死亡做出的卓越贡献,巴斯德获得了共和国所能给予的一切荣誉,如去世后,人们为其举行了国葬。在巴黎,巴斯德都有以他名字命名的研究所、大道和地铁站。即使在今天的法国,每个村庄都有以他的名字命名的广场、街道和林荫路。在法兰西共和国的集体意识中,疫苗已经成为了进步的化身。巴斯德的研究已经深深印在了法国人的脑海中。巴黎以及遍布世界的巴斯特研究院,为传播科学做出了巨大贡献,创造了世上疫苗接种的伟大史诗。

巴斯德创立的研究体系成果产出丰沛,他的“后继者”们紧接着在巴黎研制出了白喉、破伤风和伤寒疫苗,在达喀尔研制出了黄热病疫苗,在里尔研制出了肺结核疫苗[3]。此外,强制疫苗接种在法国出现的时间相对较晚:1904年实行天花疫苗接种(英国是1853年),1938年实行白喉疫苗接种,1940年实行破伤风疫苗接种, 1950年实行卡介苗(卡尔梅特( Calmette)和介朗( Guérin)发明的结核病疫苗)接种,1964年实行脊髓灰质炎疫苗接种。而在1984年和2007年取消天花疫苗和卡介苗疫苗的强制接种。由此可见,疫苗的抵制活动直到20世纪下半叶才开始在法国活跃起来。
1.5. 疫苗的现状
如今发达国家对疫苗的质疑声依旧不断。这其中原因众多[4]:首先,在不到一代人的时间内,发达国家传染病感染减退(得益于疫苗的成功)以至于人们的恐慌几乎已消失殆尽;其次,现代流行病学研究显示,疫苗(像其他药物一样)可能会产生副作用,引起民众担忧;最后,疫苗注射的对象是健康人群,在此背景下,疫苗产生不良反应让人难以接受;更有甚者,怀疑政策制定者和疫苗制造商之间存在利益冲突或勾结。因此,对疫苗的抵抗愈演愈烈,尤其是在法国。2016年发表的一项关于公众对疫苗信任度的研究显示,法国民众对疫苗缺乏信任度,在各国家中比例最高[5]。研究表明,在法国,有41%的受访者不相信疫苗,该比例高于波斯尼亚和黑塞哥维那(36%),而国际平均不信任比例只有13%。法国政府为此忧心忡忡,近年来,为了达到疫苗接种覆盖率指标,法国已经发布了几份关于疫苗接种政策的议会报告。同时,政府发起了一场全国性对话,并于2016年底提交了报告[6]。报告建议,将婴幼儿强制性接种的疫苗增加为11种,即著名的“11种疫苗”法令。该法令从2018年1月生效。
2. 对疫苗的抵制和争议
2.1. 从旧时的事故到如今的严重后果
[来源:美国出生缺陷基金会,通过维基共享]
反对疫苗的言论是基于一些真实发生的历史事件,这些事件发生在还缺乏工业生产标准的时代,如20世纪30年代在德国发生的“吕贝克(Lübeck)”事故。当时,卡介苗被一支结核毒株污染,导致接种的251名儿童中72人死亡。1955年出现了卡特实验室事故,当时卡特实验室生产了第一批由乔纳斯·索尔克发明的脊髓灰质炎灭活疫苗。仅仅不到两周,加州的卡特实验室投放出几批灭活过程控制不佳的疫苗。结果接种的儿童中,56名儿童患上了小儿麻痹症,5人丧生。同时,病毒传染给患儿的家人,最终增加了116例麻痹性脊髓灰质炎病例,5例死亡病例。这是一个惨重的教训,厂家开始意识到控制质量的重要性。除了这些广为人知的事件,近些年来现代疫苗引发的争议要么是未经证实、缺乏科学依据的分析,要么是真实的渎职案例。
2.2. 乙型肝炎疫苗:以法国为例
乙型肝炎是一个重大的公共卫生问题。在今天的法国,有近28万人患有慢性乙型肝炎,每年造成1500人死亡。全球估计有20亿人感染了这种病毒(几乎占世界人口的三分之一),根据世界卫生组织的统计,2016年有2.57亿人感染了慢性乙型肝炎,导致了 88.7万人死亡。乙型肝炎主要通过性传播、血液传播以及母婴传播(40%~90%的病例都是因未经治疗而感染)。病毒通过感染肝脏,引起急性肝炎 (临床上表现为黄疸),还有极少数情况下引起暴发性肝炎:肝细胞坏死,肝移植是唯一的治疗方法。5%的病例并发慢性肝炎,其病毒会持续存在于血液中。慢性乙型肝炎会在数月甚至数年内缓慢发展成肝硬化和肝癌。乙肝病毒的传染性极强,是人类免疫缺陷病毒(HIV)的 50至 100倍。它可以通过被血迹污染的日常工具(如指甲钳、剃须刀、耳环等),或一些专业场所(针灸馆、刺青店、美容院等)中消毒不良的器具传播。在1990年的法国,每年估计有超过2万例的新增感染病例。
因此,法国决定发起对婴幼儿、青少年和成人等易感人群的乙肝疫苗接种运动。有报道称,有青年人接种乙肝疫苗后,患上多发性硬化症的神经系统疾病。于是,一些协会成立起来组织这些病人诉诸法庭。1998年,法国健康产品卫生安全局( AFSSAPS,现改名为ANSM,即国家药品与保健产品安全局)开展了相关的科学研究。这种与乙肝疫苗关联的神经系统疾病病例,除了法国,其他地方均无报道。1998年秋,在媒体和相关协会的压力下,法国卫生部长决定暂停六年级青少年的乙肝疫苗的接种。但随后一切研究都表明乙肝疫苗接种和多发性硬化症之间没有生物学相关性。由于乙肝疫苗接种时期,正是在年轻人多发性硬化症自然发病期间,所以这些病例的出现只是某种巧合,并不能说明这两者具有因果关系。根据药物耐受数据和药物不良反应数据,以及30多年来的随访[7] [8],乙肝疫苗的安全性得以肯定。到目前为止,已经安全注射数十亿剂乙型肝炎疫苗。而青年时期正是性接触风险较高的年龄段,暂停接种疫苗相当于让其完全暴露在乙肝病毒之下。法国1998年暂停对青少年进行乙肝疫苗接种对公共健康产生了不利影响。据估计,继续为这些青少年接种疫苗,每年可预防1000例急性肝炎、100例慢性肝炎和 5例重型肝炎。就乙肝疫苗而言,由于过度防范,人体内的健康警报导致了免疫混乱(见焦点预防原则)。
2.3. 法国疫苗中的铝佐剂

免疫佐剂是疫苗中与抗原一起使用的辅助物质。佐剂能够刺激或加强抗原的特异性免疫反应而不诱导针对自身的免疫反应。
自1998年以来,法国国内对疫苗中使用铝作为佐剂是否安全一直争论不休。罗曼·热拉尔迪( Romain Gherardi)教授在著名医学期刊《柳叶刀》上发表的一篇文章一石激起千层浪。该文章描述了18例患者罹患一种新型肌肉疾病 :巨噬细胞肌筋膜炎[9]。研究表明,在患者身上观察到的微疤痕与体内出现的铝有关,而这些铝很有可能是肌肉注射疫苗的残留物。 2003年,罗曼·热拉尔迪的研究团队将巨噬细胞肌筋膜炎与一种更广泛的综合征慢性疲劳综合征联系起来[10] [11]。而被质疑的疫苗正是20世纪90年代在成年人群中广泛接种的抗乙肝疫苗。
然而,这项研究的结果从几个方面来看都疑点重重:
- 首先,自1925年以来,铝就一直被用作疫苗的佐剂,从一开始便有数百亿剂疫苗被接种。同时,全球还采集了大量实验数据保证其安全性。那么,铝作为佐剂安全性下降后果是巨大的,因为全球已接种了上百亿剂疫苗。
- 其次,该肌肉综合征仅仅只是在法国出现,更确切地说,只在克雷代伊团队中的患者中发现。
- 最后,大量接触含铝佐剂疫苗的是儿童,而这批病患却仅由成年人组成。
尽管真假难辨,铝佐剂的问题还是受到了法国卫生机构的长期关注。 1999年,世界卫生组织(WHO)成立了一个疫苗安全咨询委员会来解决疫苗的安全问题,其中第一个要解决的便是铝佐剂问题。法国国家公共健康监督学会( INvS)于2002年启动了有关药物不良反应的研究。此后,关于铝佐剂的报告层出不穷:2012年法国国家医学科学院报告,2013年法国公共卫生高级委员会报告,2014年科学技术选择评估议会办公室报告,2016年法国国家药学科学院报告。药学科学院的报告指出,“鉴于与组织学病变相关的临床表现的异质性和非特异性,不可能定义巨噬细胞肌筋膜炎综合征”[12],出现肌肉疾病的病例只是少数,甚至是唯一的病例[13],这可能与特殊的遗传倾向有关。 法国国家医疗健康产品安全局(ANSM)提醒到,在任何情况下,疫苗潜在的危险与其能带来的好处完全不能相提并论。
2.4. 硫柳汞与自闭症
硫柳汞是一种有机汞化合物,也是一种生物杀灭活性物质 (即能杀死污染微生物)。硫柳汞还能提高药物稳定性。这些特性适用于多人份包装的疫苗(一瓶疫苗用于多人接种)。由于多人份包装疫苗不会同时给几个病人注射,所以通过添加硫柳汞,疫苗就可以打开后一直使用,而不会被污染。
1999年,在美国,开始出现硫柳汞与儿童神经发育缺陷有关的传闻[14]。这些担忧源自婴幼儿疫苗接种计划中注射的汞含量累计超过了美国官方建议的最大量。但是从毒理学的角度来看,这些疫苗所含硫柳汞的含量微乎其微,比例为 0.003%~0.01%,即每剂量最大含量为 25~50µg。在这样的剂量下,理论上讲没有任何毒性风险的。
即便如此,食品和药物监管局( FDA)还是要求儿童疫苗中不再使用硫柳汞,2001年在美国和欧洲开始实施。2007年,发表在《新英格兰医学杂志》(New England Journal of Medicine)上的系列完善的科学研究表明,硫柳汞与自闭症障碍之间没有联系[15]。
许多机构再一次关注硫柳汞问题。世界卫生组织在2006年、欧洲药品管理局( EMA)在 2007年和法国健康产品卫生安全局(AFSSAPS)在 2009年一致认为,使用硫柳汞会对神经系统造成危害未经证实 (即使无法从科学上排除 )。鉴于硫柳汞是多剂次疫苗的不可或缺的防腐剂,使用硫柳汞的好处大于理论上的毒性风险。
2.5. 小儿麻痹症疫苗和艾滋病疫苗
1999年,一本书引发了另一场争论。据报道,1959年在非洲使用的口服脊髓灰质炎疫苗可能导致了艾滋病毒的大流行[16]。缘由是该疫苗进入人体后,会产生含有猴免疫缺陷病毒( SIVcpz)的黑猩猩肾细胞,使人感染上 M组免疫缺陷病毒( HIV),患上全球获得性免疫缺陷综合征( AIDS)大流行。然而,这种疫苗通常是在不携带黑猩猩SIV病毒的绿猴肾细胞(Vero细胞)上生产的。
通过对病毒的分子比较研究后,这一假设很快遭到了否定[17] [18],艾滋病病毒并非来自口服脊髓灰质炎疫苗。同时,有关艾滋病病毒出现的最新数据也证实了这一结果:早在 1959年以前,艾滋病病毒就已经在刚果河的两岸出现,在20世纪30年代,非洲的金沙萨就已经出现过该病毒的踪影[19]。
2.6. 疫苗过度接种的说法
当谣言一个一个在科学面前不攻自破后,出现了其他对疫苗更加恶毒的攻击。
反对疫苗的自然主义派宣扬“生病好过接种疫苗”,随后又出现了“疫苗导致免疫系统疲惫,从而让人生病”的说法。多次接种疫苗可能会导致免疫系统的过度激活。
这种观点其实是一种谬论。
- 一方面,我们的疫苗已经不断被精炼。据估计,20年前接种计划中的所有疫苗中大约有3000种抗原。而到了现在,抗原的数量已经减少到150[20]。在这之前我们必须了解,种或150种抗原相对于我们周围10万亿个细菌和病毒来说只是沧海一粟。从出生以来,我们的免疫系统就一直在对这些细菌和病毒做出响应。这代表接种疫苗只是人类进化过程中免疫系统获得的微不足道的一次冲击。因此,免疫接种后,我们的免疫系统也远远没有达到[21]的过度饱和的状态。
- 另一方面,现代免疫学告诉我们,环境对免疫系统的刺激是免疫协调发展的必要条件[22](参见人类微生物群:我们健康的盟友)。
3. 什么样的公共卫生政策?
3.1. 疫苗的益处
从流行病学的角度来看,疫苗书写了一段成功的故事。在 20世纪的美国,通过疫苗预防的疾病的发病率下降了100%[23],法国也是类似的结果。最后的本土小儿麻痹症和白喉病例出现在1989年。由于破伤风病菌的孢子抵抗不良环境的能力强,可以在土壤中永久存在,因此无法根除,但每年病例数控制在十几例以下。自从1992年开始接种 b型流感嗜血杆菌疫苗以来,5岁以下儿童的脑膜炎发病率下降了96%[24]。
疫苗不仅限于减少病患数量,还可以让人类获得意想不到的好处。比如麻疹疫苗不仅可以减少麻疹相关的死亡率,还能在延长人的寿命[25]。这种附加的好处是因为麻疹病毒具有高度免疫抑制作用,会使人体对其他很多疾病失去免疫力,疫苗通过保护我们免受麻疹的感染,也相当于提高了我们对其他疾病的抵御能力。
肺炎球菌是一种导致耳部感染、脑膜炎和严重肺部感染的细菌,多见于儿童和老年人。将肺炎球菌疫苗的接种纳入儿童免疫计划中,不仅大大减少了儿童的耳部感染和脑膜炎的发生率,而且同时减少了(未接种疫苗的)老年人的肺炎的感染率,这向我们传递了一个信息:儿童是老年人肺炎球菌的传染媒介。通过给儿童接种疫苗来阻断肺炎球菌的传播,不仅能直接保护儿童,还能间接保护他们身边的老年人。疫苗的存在使儿童预防了疾病的早期感染,减少药物的使用,避免抗生素耐药,降低家庭医疗开支。
总而言之,疫苗接种可以降低感染机率。但是,得到控制的传染病并没因此而完全消失,他们静候疫苗“保护盾”出现纰漏,以便卷土重来。
3.2. 疫苗接种覆盖率下降带来的实际效应
1900年,法国人的平均寿命约为 45岁。而到2016年,法国男性和女性的平均寿命分别达到了79.4岁和85.4岁。虽然疫苗不是人均寿命大幅增加的唯一原因,但其巨大贡献不言而喻。
疫苗接种率降低,就像钟摆一样,导致可怕的百日咳、白喉卷土重来(随着苏联帝国的解体,在俄罗斯重新出现),还有幼儿脑膜炎、麻疹、腮腺炎、风疹都曾重新出现过,脊髓灰质炎也曾重现欧洲。并且大量使用抗生素治疗病毒感染的细菌并发症后,最终导致抗生素耐药性增加。

最近的一个典型的例子就是法国2008年至2012年的麻疹疫情[26] [27]。麻疹是已知传染病中传染性最强的疾病。1983年,麻疹疫苗接种已经纳入法国免疫接种计划名录中( MMR疫苗),从1996年开始建议注射第二针(第一针注射一年之后)。2002年,世界卫生组织提出了2010年前在欧洲地区域根除麻疹。这一目标意味着要将麻疹发病率(相对于人口的患病人数)维持在每百万人不到1例的水平。目标的实现要依靠群体免疫,群体免疫是流行病学中的一种防疫机制,当有足够比例的人群接种疫苗时,传染病在人群中的传播就会被抑制(图 5)。一旦有输入性病例,病毒如瓮中之鳖,无处遁形,自取灭亡。
法国在2005年启动了一项麻疹计划,麻疹病例必须上报,并对上报病例进行流行病调查。法国2006年度麻疹病例已经不到 50例,低于世界卫生组织设定的目标。可惜的是,由于麻疹接种覆盖率下降,2008年初麻疹又卷土重来。2008至2012年间发现了 23000人感染麻疹,近 5000人住院(1023名患有严重的病毒性肺炎或细菌性肺炎, 27名患有神经系统并发症如脑炎或脊髓炎), 10人死亡(大多数人年龄在30岁以下)。由于法国麻疹疫苗接种覆盖率不足,建模研究也同样预测出了这场可怕的故态复萌。虽然近年来法国婴幼儿MMR联合疫苗的接种覆盖率有所提高,但仍然不足。世界卫生组织计划的目标是每年疫苗接种的第一针和第二针覆盖率分别要达到 95%和 80%,而法国第一针疫苗的接种率为90%,第二针则跌落至54%。
这告诉我们,只有在世界范围内消除麻疹,我们才能真正对这种疾病降低防范。这是一项长期而复杂的任务,小儿麻痹症已实现此目标,脊髓灰质炎正在进行中,麻疹也在计划中。这需要全球的共同协调和努力,消灭一种病毒就像割断一条链条一样,取决于它最薄弱的环节。
3.3. 强制接种还是自愿接种?
法国和意大利是欧盟国家中最后两个实施强制疫苗接种的国家。这是 20世纪中叶历史选择的结果,当时传染病仍对这两个国家危害巨大。作为立法者,国家需要在传染病的危急关头有效防治疾病。但1964年以来,没有任何新的疫苗被列入强制接种的计划中。这也与社会变化有关,在当时的法国社会,患者更多的是自己做选择。强制接种似乎与2002年3月4日法国颁布的关于患者权利的法令,特别是患者有拒绝接受治疗的权利的法令相抵触。疫苗接种政策缺乏明确性,遭到疫苗接种反对者的诟病。
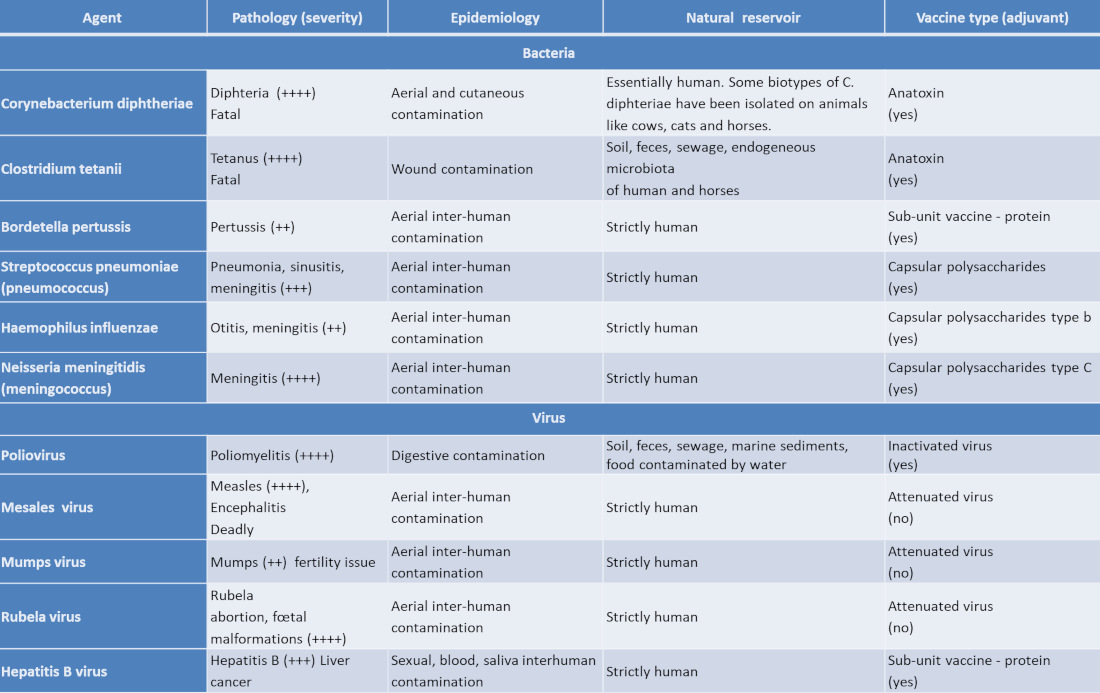
强制接种疫苗显得无关紧要,因为它们预防的是在法国已经消失的疾病(如白喉、脊髓灰质炎 ),而自愿接种如乙型肝炎疫苗和人类乳头瘤病毒疫苗,每年则可以分别保护1,500人和1,000人免遭死亡威胁。而强制性疫苗和自愿接种疫苗之间的区别对待导致民众以为自愿接种的疫苗并不重要。这种想法最直接的体现是疫苗接种覆盖率,在官方的儿童接种计划中,建议接种的11种疫苗只有 3种是强制性的(见表)。
不育的睾丸炎和孕妇胎儿的病变 )。以及,接种乙肝疫苗也显著降低了肝癌的发病率。
(Agent传染源; Pathology (severity)病理学 (严重程度 );Epidemiology 流行病学; Natural reservoir自然宿主; vaccine type (adjuvant)疫苗类型 (辅助);Corynebacterium diphtheriae白喉杆菌; Clostridium tetanii破伤风梭状芽胞杆菌; Bordetella pertussis百日咳博德特氏菌; Streptococcus pneumoniae (pneumococcus)链球菌引起的肺炎 (肺炎球菌 ); Haemophilus influenzae 流感嗜血杆菌; Neisseria meningitidis (meningococcus)脑膜炎奈瑟氏菌 (脑膜炎球菌);Rubela 风疹; Fatal致命的; Tetanus破伤风; Pertussis 百日咳; Pneumonia, 肺炎; sinusitis,鼻窦炎; meningitis脑膜炎; Otitis耳炎; meningitis脑膜炎; Meningitis脑膜炎; Poliomyelitis小儿麻痹症; Measles 麻疹; Encephalitis脑炎; Mumps流行性腮腺炎; fertility issue生育问题; abortion, 堕胎; malformations畸形; Hepatitis B乙型肝炎; Liver cancer肝癌; Diphteria白喉; Aerial and cutaneous contamination空气传播和皮肤感染; Wound contamination创口感染; Aerial inter-human contamination空气传播和体液传播; Digestive contamination消化道感染; Sexual, blood, saliva inter human contamination性传播、母婴传播和体液传播; human人类; Some biotypes of C.diphteriae have been isolated on animals like cows, cats and horses 在牛、猫和马等动物身上分离出了一些白喉分枝杆菌的生物型; Soil, feces, sewage, endogeneous microbiotaof human and horses土壤,粪便,污水,人和马的内生微生物; Strictly human严格的人体内; Anatoxin 类毒素; Sub-unit vaccine -protein 亚单位疫苗蛋白; Capsular polysaccharides 荚膜多糖; Capsular polysaccharides type b b型荚膜多糖; Inactivated virus 灭活病毒; Attenuated virus减毒病毒;)
据世界卫生组织统计,比起欧洲其他国家,法国自愿接种疫苗的覆盖率要较低。如2012年,法国2岁儿童乙肝疫苗接种率为74%,德国超过86%,比利时和西班牙为 96%,这三个国家都没有实行强制疫苗接种。 2012年法国审计法院提交了一份关于法国疫苗接种政策的成本和有效性的报告,并构成2013年乔治斯( Georges Labazée)为参议院社会事务委员会(Senate Social Affairs Committee)所做的报告的一部分。 2014年,法国公共卫生高级委员会( HCSP)发布了关于疫苗接种政策的意见,建议卫生当局组织辩论规定疫苗接种义务。2015年,卫生部长将义务接种问题提交给参议员桑德琳·胡雷尔(Sandrine Hurel)。其在 2016年提交的报告也呼吁改变法国地区的疫苗接种现状,并就疫苗接种问题进行重大磋商,以确定法国准备冒着何种集体风险来消除个人限制。2016年,阿兰·费舍尔( Alain Fischer)教授主持召开了疫苗接种的磋商会议。2016年 11月 30日递交给部长的会议报告建议,将疫苗接种义务暂时扩展到免疫接种计划中所有自愿接种的疫苗 (增加个人有权利拒绝疫苗接种的豁免条款 ),同时长期保留解除接种义务的可能性(一旦民众对疫苗恢复信任)[6]。正是本着这种精神,法国政府在2017年夏季宣布法国的婴幼儿必须接种11种疫苗。准确地说,不是11种疫苗,而是四联疫苗(多价型疫苗),儿童仅需要接种4次,可以预防11种严重疾病。
参考资料及说明
封面图片:以宿存孢子的形式存在的破伤风杆菌(计算机生成的图像)[无版权]
[1] Moulin A-M. L’aventure de la vaccination. Paris: Fayard; 1996. 498 p. (in french)
[2] Swales JD. The Leicester anti-vaccination movement. Lancet. 1992;340(8826):1019-21
[3] Perrot A, Schwartz M. Pasteur et ses lieutenants: Roux, Yersin et les autres, Odile Jacob; 2013. 270 p. (in french)
[4] Floret D. Les résistances à la vaccination. Med Sci (Paris). 2010;26(12):1087-93
[5] Larson HJ, de Figueiredo A, Xiahong Z, Schulz WS, Verger P, Johnston IG, et al The State of Vaccine Confidence 2016: Global Insights Through a 67-Country Survey. EBioMedicine. 2016;12:295-301
[6] Fischer A. (dir.) Rapport sur la vaccination – Comité d’orientation de la concertation citoyenne sur la vaccination, novembre 2016. Paris Ministère des Affaires sociales et de la Santé ; 2016. 502p. http://www.ladocumentationfrancaise.fr/rapports-publics/164000753/index.shtml (in french)
[7] Launay O, Floret D. Vaccination against Hepatitis B: What’s Up? Rev Prat. 2015;65(7):953-61
[8] Launay O, Floret D. Hepatitis B vaccination: a review. Med Sci (Paris). 2015;31(5):551-8
[9] Gherardi RK, Coquet M, Cherin P, Authier FJ, Laforet P, Belec L, et al. Macrophagic myofasciitis: an emerging entity. Groupe d’Etudes et Recherche sur les Maladies Musculaires Acquises et Dysimmunitaires (GERMMAD) de l’Association Francaise contre les Myopathies (AFM). Lancet. 1998;352(9125):347-52
[10] Gherardi RK. Lessons from macrophagic myofasciitis: towards definition of a vaccine adjuvant-related syndrome. Rev Neurol (Paris). 2003;159(2):162-4
[11] Gherardi RK, Authier FJ. Aluminum inclusion macrophagic myofasciitis: a recently identified condition. Immunol Allergy Clin North Am. 2003;23(4):699-712
[12] Les adjuvants aluminiques : le point en 2016. Académie de pharmacie; 2016 (in french) Encyclopédie de l’environnement 13/13 Généré le 13/08/2021
[13] Van Der Gucht A, Aoun Sebaiti M, Guedj E, Aouizerate J, Yara S, Gherardi RK, Evangelista E, Chalaye J, Cottereau AS, Verger A, Bachoud-Levi AC, Abulizi M, Itti E, Authier FJ Brain 18F-FDG PET Metabolic Abnormalities in Patients with Long-Lasting Macrophagic Myofascitis J Nucl Med. 2017 Mar;58(3):492-498. doi: 10.2967/jnumed.114.151878. Epub 2016 Oct 20.
[14] Grandjean P, White RF. Effects of methylmercury exposure on neurodevelopment. JAMA. 1999;281(10):896; author reply 7
[15] Thompson WW, Price C, Goodson B, Shay DK, Benson P, Hinrichsen VL, et al. Early thimerosal exposure and neuropsychological outcomes at 7 to 10 years. N Engl J Med. 2007;357(13):1281-92
[16] Hopper E. The River: A Journey to the Source of HIV And AIDS: Lippincott Williams and Wilkins; 1999. 1070 p.
[17] Worobey M, Santiago ML, Keele BF, Ndjango JB, Joy JB, Labama BL, et al. Origin of AIDS: contaminated polio vaccine theory refuted. Nature. 2004;428(6985):820.
[18] Plotkin SA. CHAT oral polio vaccine was not the source of human immunodeficiency virus type 1 group M for humans. Clin Infect Dis. 2001;32(7):1068-84.
[19] Faria NR, Rambaut A, Suchard MA, Baele G, Bedford T, Ward MJ, et al. HIV epidemiology. The early spread and epidemic ignition of HIV-1 in human populations. Science. 2014;346(6205):56-61.
[20] Sansonetti P. Vaccins. Odile Jacob ; 2017. 222 p. (in french)
[21] Gregson AL, Edelman R. Does antigenic overload exist? The role of multiple immunizations in children. Immunol Allergy Clin North Am. 2003;23(4):649-64.
[22] Gomez de Aguero M, Ganal-Vonarburg SC, Fuhrer T, Rupp S, Uchimura Y, Li H, et al The maternal microbiota drives early postnatal innate immune development. Science. 2016;351(6279):1296-302.
[23] van Panhuis WG, Grefenstette J, Jung SY, Chok NS, Cross A, Eng H, et al. Contagious diseases in the United States from 1888 to the present. N Engl J Med. 2013;369(22):2152-8
[24] Georges S, Lepoutre A, Dabernat H, Levy-Bruhl D. Impact of Haemophilus influenzae type b vaccination on the incidence of invasive Haemophilus influenzae disease in France, 15 years after its introduction. Epidemiol Infect. 2013;141(9):1787-96.
[25] Mina MJ, Metcalf CJ, from Swart RL, Osterhaus AD, Grenfell BT. Long-term measles-induced immunomodulation increases overall childhood infectious disease mortality. Science. 2015;348(6235):694-9
[26] Floret D. Measles vaccination. Rev Prat. 2010; 60(10):1368-70.
[27] Antona D, Levy-Bruhl D, Baudon C, Freymuth F, Lamy M, Maine C, et al Measles elimination efforts and 2008-2011
环境百科全书由环境和能源百科全书协会出版 (www.a3e.fr),该协会与格勒诺布尔阿尔卑斯大学和格勒诺布尔INP有合同关系,并由法国科学院赞助。
引用这篇文章: TOURNIER Jean-Nicolas (2024年3月10日), 疫苗,防御病原体的有效措施, 环境百科全书,咨询于 2026年7月29日 [在线ISSN 2555-0950]网址: https://www.encyclopedie-environnement.org/zh/sante-zh/vaccines-proven-protection-against-pathogens-environment/.
环境百科全书中的文章是根据知识共享BY-NC-SA许可条款提供的,该许可授权复制的条件是:引用来源,不作商业使用,共享相同的初始条件,并且在每次重复使用或分发时复制知识共享BY-NC-SA许可声明。